
Oedema
Table of Contents
Definition of edema
edema may be defined as abnormal and excessive accumulation of “free fluid” in
the interstitial tissue spaces and serous cavities.
Types of edema
The edema may be of 2 main types on the basis of location:
- Localised when limited to organ or limb e.g. lymphatic edema, inflammatory edema, allergic edema.
- Generalised (anasarca or dropsy) when it is systemic i distribution, particularly noticeable in the subcutaneous tissues e.g. renal edema, cardiac edema, nutritional edema.
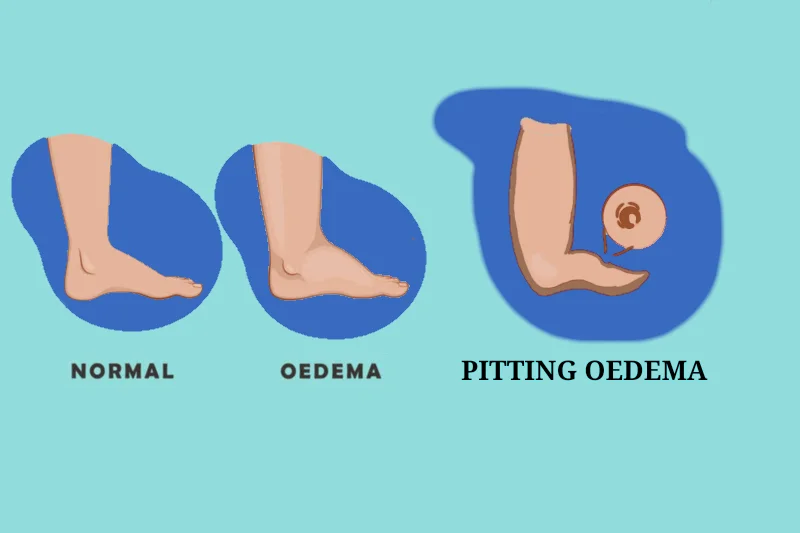
There are 2 types of edema on the basis of fluid filled edema
- pitting edema
- non – pitting edema
There are a few special forms of edema .Depending upon fluid composition, edema fluid may
be:
- Transudate which is more often case, such as in edema of cardiac and renal disease; or
- Exudate such as in inflammatory edema.
Pathogenesis of Oedema
Oedema is caused by mechanisms that interfere with normal fluid balance of plasma, interstitial fluid and lymph flows. The following mechanisms may be operating singly or in combination to produces oedema:
- Decreased plasma oncotic pressure
- Increased capillary hydrostatic pressure
- Lymphatic obstruction
- Tissue factors (increased oncotic pressure of interstitial
fluid, and decreased tissue tension) - Increased capillary permeability
- Sodium and water retention.
Causes of oedema
- Allergic reaction, urticaria, and angioedema
- Cardiac disease
- Hepatic disease
- Renal disease
- Malabsorption/protein-calorie malnutrition
- Obstructive sleep apnea
- Pregnancy and premenstrual oedema
- Cellulitis
- Chronic venous insufficiency
- Compartment syndrome
- Complex regional pain syndrome type 1 (reflex sympathetic dystrophy)
- Deep venous thrombosis
- Iliac vein obstruction
- Lipedema
- Lymphedema(lymphedema Primary: congenital lymphedema,
lymphedema praecox, lymphedema tarda ) - Secondary: from axillary lymph node dissection, surgery (e.g., coronary artery bypass graft, inguinal lymphadenectomy) trauma, tumor, radiation, filariasis
- May-Thurner syndrome (compression of left iliac vein by right iliac artery)
Pathogenesis and Morphology of important types of edema
Renal Oedema
- edema in nephrotic syndrome
The nephrotic edema is classically more severe and marked and is present in the subcutaneous tissues as well as in the visceral organs. The affected organs is enlarged and heavy with tense capsule.
Microscopically
The oedema fluid separates the connective tissue fibres of subcutaneous tissues. Depending upon protein content, the oedema fluid may appear homogeneous, pale, eosinophilic, or may be deeply eosinophilic and granular.
- Oedema in nephritic syndrome
Oedema occurs in condition with diffuse glomerular disease such as in acute diffuse glomerulonephritis and rapidly progressive glomerulonephritis (nephritic oedema). The nephritic oedema is usually mild as compared to nephrotic oedema and begins in loose tissues such as on
the face around eyes, ankles and genitalia. edema in these conditions is usually not affected by gravity.
- Oedema in acute tubular injury
Acute tubular injury following shock or toxic chemical results in gross edema of body.
Cerebral Oedema
Cerebral oedema or swelling of brain is most threatening
example of edema. Cerebral oedema can be of 3 types:
VASOGENIC OEDEMA
Vasogenic edema is prominent around cerebral contusions, infarcts, brain abscess and some tumors.
Grossly, the white matter is soft, swollen, with flattened gyri and narrowed sulci.
Microscopically, there is separation of tissue elements by oedema fluid and swelling of astrocytes. The perivascular (Virchow-Robin) space is widened and clear halos are seen around small blood vessels.
CYTOTOXIC OEDEMA
In this type, the blood-brain barrier is intact and the fluid accumulation is intracellular, occurs in some metabolic derangements, acute hypoxia and with some toxic chemicals.
Microscopically, the cells are swollen and vacuolated. In situations, both vasogenic as well as cytotoxic cerebral oedema results e.g. in purulent meningitis.
INTERSTITIAL OEDEMA
This type of cerebral oedema occurs when excessive fluid crosses the ependymal lining of ventricles and accumulates in periventricular white matter.
Hepatic Oedema
Oedema of legs and ascites in cirrhosis of liver is as under:
- There is hypoproteinemia due to impaired synthesis of proteins by the diseased liver
- Due to portal hypertension, there is increased venous pressure in abdomen, and hence raised hydrostatic pressure.
- Failure of inactivation of aldosterone in diseased liver and hence hyperaldosteronism
- Secondary stimulation of renin-angiotensin mechanism promoting sodium and water retention.
Nutritional Oedema
Oedema due to nutritional deficiency of proteins ( prolonged starvation, famine, fasting), vitamins (beri-beri due to vitamin B1 deficiency) and chronic alcoholism occurs on
legs but sometimes may be more generalised.
Myxedema
Myxedema from hypothyroidism is a form of non-pitting oedema occurring on skin of face and other parts of the body as also in the internal organs due to excessive deposition of glycosaminoglycans in the interstitium.

Diagnosis of Common Causes of Localized oedema
Unilateral predominance( means in one side of body) Bilateral predominance (means both side of body ) | Onset and location | Examination findings |
| Chronic venous insufficiency | Onset: chronic; begins in middle to older age Location: lower extremities; bilateral distribution in later stages | Soft, pitting oedema with reddish-hued skin; predilection for medial ankle/calf. Associated findings: venous ulcerations over medial malleolus; weeping erosions |
| Complex regional pain syndrome type 1 (reflex sympathetic dystrophy) | Onset: chronic; following trauma or other inciting event Location: upper or lower extremities; contralateral limb at risk regardless of trauma | Soft tissue oedema distal to affected limb Associated findings: (early) warm, tender skin with diaphoresis; (late) thin, shiny skin with atrophic changes |
| DVT | Onset: acute Location: upper or lower extremities | Pitting oedema with tenderness, with or without erythema; positive Homans sign |
| Lymphedema | Onset: chronic; insidious; often following lymphatic obstruction from trauma or surgery Location: upper or lower extremities; bilateral in 30% of patients | Early: dough-like skin; pitting Late: thickened, verrucous, fibrotic, hyperkeratotic skin Associated findings: inability to tent skin over second digit, swelling of dorsum of foot with squared off digits, painless heaviness in extremity |
| Lipedema | Onset: chronic; begins around or after puberty Location: predominantly lower extremities; involves thighs, legs, buttocks; spares feet, ankles, and upper torso | Nonpitting oedema; increased distribution of soft, adipose tissue Associated findings: medial thigh and tibial tenderness; fat pad anterior to lateral malleoli |
| Medicationinduced oedema | Onset: weeks after initiation of medication; resolves within days of stopping offending medication Location: lower extremities | Soft, pitting oedema |
| Obstructive sleep apnea | Onset: chronic Location: lower extremities | Mild, pitting oedema Associated findings: daytime fatigue, snoring, obesity |
Diagnostic testing
- Ultrasonography
- lymphoscintigraphy
- MRI
Management of oedema
Management of oedema should be on the basis of etiology .
Chronic venous insufficiency
1. Mechanical therapies, including leg elevation and compression stockings with 20 to 30 mm Hg for mild edema and 30 to 40 mm Hg for severe edema
complicated by ulceration, are recommended.
2.Compression therapy is contraindicated in patients with peripheral arterial disease. A study of 120 patients with venous ulcers showed that 6% had mixed arterial-venous ulcers.
3. Treatment includes daily hydration with emollients and short courses of topical steroid creams for severely inflamed skin.
lymphedema
1. Treatment includes compression stockings at 30 to 40 mm Hg.
2.Pneumatic compression devices have been shown to augment standard therapies. Women with breast cancer– related lymphedema showed statistically significant improvement in lymphatic function following one hour of pneumatic compression therapy.In a study of 155
patients with cancer- and non–cancer-related lymphedema, 95% of patients noted reduction in limb oedema
after using pneumatic compression devices at home.
3.Diuretics do not have a role in the treatment of lymphedema.
DVT(Deep venous thrombosis )
Anticoagulation therapy (unfractionated or low-molecular-weight heparin or warfarin [Coumadin]).Anticoagulation, compression stockings should be used after a DVT to prevent post thrombotic syndrome.

Medication-induced oedema
In patients taking calcium channel blockers to treat hypertension, use of angiotensin-converting enzyme inhibitor may be more beneficial than angiotensin receptor blocker therapy in reducing calcium channel blocker–induced peripheral oedema.
Other causes
1.There is no treatment for lipedema. Weight loss does not affect this condition.
2. Complex regional pain syndrome is treated with physical therapy in combination with medications such as systemic steroids and tricyclic
antidepressants.
3.Obstructive sleep apnea is treated with positive pressure ventilation.