
Polyneuropathy : Physical examination
Table of Contents
Sensory Examination
1.Light touch examination
This test using a wisp of cotton wool in area of total loss of sensation. In polyneuropathy ,sensory loss is symmetrical and follow a characteristic stocking and glove distribution.

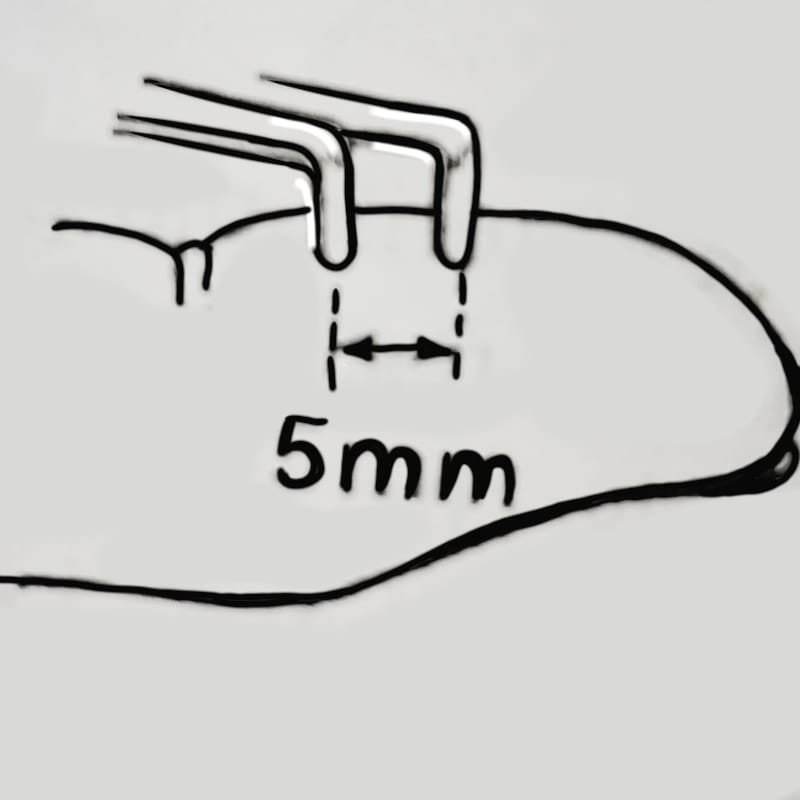
2.Two point discrimination
In Polyneuropathy ,Two point discrimination help to test the ability to discriminate two blunt points when simultaneously applied to the finger, 5mm apart .
3. Vibration
Place vibrating tuning fork (usually 128 c/s ) on a bony prominence, e.g. radius. Ask the patient to indicate when vibration, if felt, ceases. If impaired, move more proximally and repeat . Vibration testing is of value in early detection of demyelinating disease and peripheral neuropathy, but otherwise is of limited benefit.

4. Joint position sense
Hold the sides of patient’s finger or thumb and demonstrate ‘up and down ‘ movements.

5. Temperature perception
Temperature testing seldom provides any additional information. If required, use cold object or hot and cold test tubes.
6. Pain perception
Pin prick with sterile pin provides a simple method of testing this important modality. Firstly, Check that the patient detects the pin as ‘sharp’,.i.e. painful, then rapidly test each dermatome in turns.
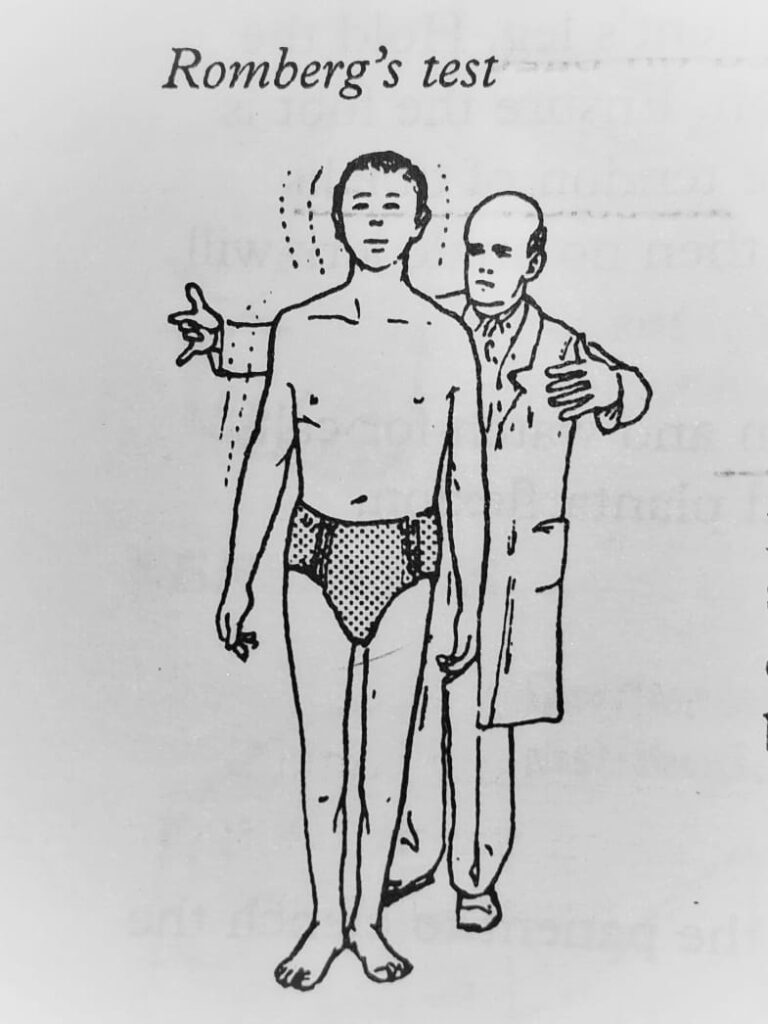
Examination of gait
Joint position impairment , sensory ataxia is evident. Romberg’s test is positive. Neuropathic burns / ulcers or joint may be present .
Tropic changes
- Cold blue extremities
- Cutaneous hair loss
- Brittle finger/toe nails occasionally occur.
Motor examination
Muscle wasting.
Evident is axonal but absent in demyelinating neuropathies . Edema of immobile limbs may mask wasting. The 1st dorsal interosseous muscle in the upper limbs and extensor digitorum brevis in the lower limbs are muscle groups. Look for fasciculations – irregular twitches of groups of muscle fibers due to diseased anterior horn cells , these may be induced by exercise or muscle percussion .
Muscle weakness.
Weakness is proportional to the number of affected motor neurons. It develop suddenly or slowly and is generally symmetrical , usually starting distally in the lower limbs and spreading to upper limbs in a similar manner before ascending into proximal muscle groups . This pattern of progression is supposedly due to ‘dying back ‘ of axons towards their nerve cells – the longest being the most vulnerable. Some neuropathies, e.g. Guillain -Barre, chronic inflammatory demyelinating polyneuropathy, may affect proximal muscle groups first.
In sever neuropathies , truncal and respiratory muscle involvement occurs. Respiratory muscle weakness may result in death.
Tendon Reflexes
The tendon reflex depends on:
- Stretch of the muscle spindle
- Activation of spindle afferent fibers
- Monosynaptic projections to the alpha motoneurons. The gamma motoneuron fibers, projecting to the spindle , ‘ modules ‘ activity in the reflex loop.
Reflexes commonly tested :
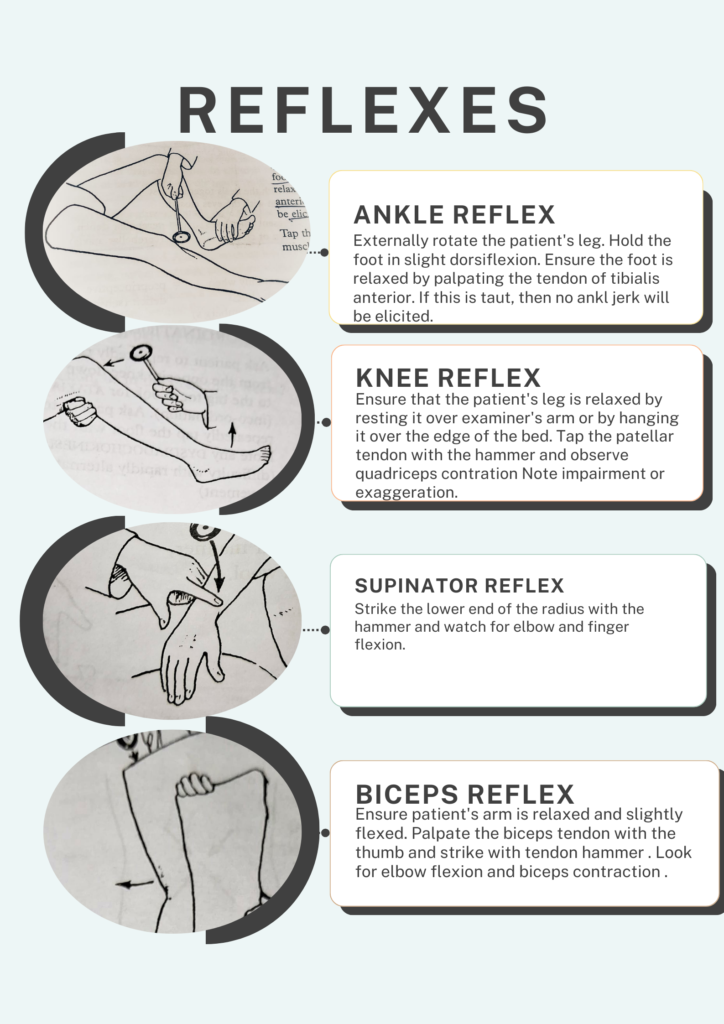
BICEPS REFLEX
Ensure patient’s arm is relaxed and slightly flexed. Palpate the biceps tendon with thumb and strike with tendon hammer . Look for the elbow flexion and biceps contraction .
SUPINATOR REFLEX
Strike the lower end of the radius with hammer and watch for elbow and finger flexion.
TRICEPS REFLEX
Strike the patient’s elbow a few inches above olecranon process. Look for the elbow extension and triceps contraction.
KNEE REFLEX
Ensure that patient’s leg is relaxed by resting it over examiner’s arm or by hanging it over the edge of the bed. Tap the patellar tendon with hammer and observe quadriceps contraction Note impairment or exaggeration.
ANKLE REFLEX
Externally rotate the patient’s leg. Hold the foot in slight dorsiflexion. Ensure the foot is relaxed by palpating tendon of tibialis anterior. If this is taut,then no ankle jerk will be elicited.
Tap the Achilleas tendon and watch for calf muscle contraction and plantarflexion.
Reference
Neurology and neurosurgery illustrated by Kenneth W Lindsay ,Page 430-444
Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd edition. Chapter – 67 Sensation.
Washington University in St .Louis , Neurological examination.