
What is AIDS?
Since the initial recognition of AIDS in the United States in 1981, tremendous advances have taken place in the understanding of this dreaded disease as regards its epidemiology, etiology, immunology, pathogenesis, clinical features and morphologic changes in various tissues and organs of the body.
EPIDEMIOLOGY
- Although AIDSwas first described in the US, the disease has now attained pandemic proportions involving all continents.
- Presently, developing countries comprise majority of cases and Africa alone constitutes 50% of all positive cases globally.
- According to a rough estimate, 1 in every 100 sexually active adults worldwide is infected with HIV.Half of all serologically positive cases are in women while children comprise 5% of all cases.
- According to the WHO data, the last decade has shown an alarming rise in incidence of AIDS cases in South-East Asia including Thailand, Indonesia and Indian sub-continent.
- In India, epicentre of the epidemic lies in the states of Maharashtra and Tamil Nadu which together comprise about 50% of all HIV positive cases (mostly contracted sexually), while North-East state of Manipur accounts for 8% of all cases (mostly among intravenous drug abusers).
AIDS is caused
AIDS is caused by an RNA retrovirus called human immunodeficiency virus (HIV) which is a type of human T cell leukaemia-lymphoma virus (HTLV)
Features
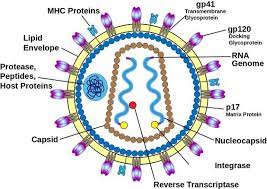
- HIV-I virion or virus particle is spherical in shape and 100- 140 nm in size.
- It contains a core having core proteins, chiefly p24 and p18, two strands of genomic RNA and the enzyme, reverse transcriptase
- The core is covered by a double layer of lipid membrane derived from the outer membrane of the infected host cell during budding process of virus
- The membrane is studded with 2 envelope glycoproteins, gp120 and gp41
- The three important genes code for the respective components of virion: gag (group antigen) for core proteins, pol (polymerase) for reverse transcriptase, and env (envelope) for the envelope proteins.
- These genes and viral components act as markers for the laboratory diagnosis of HIV infection
TRANSMISSION OF AIDS
1. Sexual transmission
Sexual contact in the main mode of spread and constitutes 75% of all cases of HIV transmission. Most cases of AIDS in the industrialised world like in the US occur in homosexual or bisexual males while heterosexual promiscuity seems to be the dominant mode of HIV infection in Africa and Asia.
2. Transmission via blood and blood products.
This mode of transmission is the next largest group (25%) and occurs in 3 groups of high-risk populations: Intravenous drug abusers, Haemophiliacs, Recipients of HIV-infected blood and blood products
3. Perinatal transmission.
HIV infection occurs from infected mother to the newborn during pregnancy transplacentally, or in immediate post-partum period through contamination with maternal blood, infected amniotic fluid or breast milk.
4. Occupational transmission
There have been a small number of health care workers (HCW), laboratory workers and those engaged in disposal of waste of sharps who have developed HIV infection by occupational exposure to HIV infected material. It is imperative that these workers follow CDC guidelines for universal precautions which include disinfecting and sterilizing all reusable devices and use of bleaching solution for disinfecting all blood spillage.
5. Transmission by other body fluids
Although besides blood, HIV has been isolated and identified from a number of body fluids such as saliva, tears, sweat and urine, semen, vaginal secretions, cervical secretions, breast milk, CSF, synovial, pleural, peritoneal and pericardial fluid, there is no definite evidence thatHIV transmission can occur by any of these fluids; isolated cases of such infection reported are in likelihood due to concomitant contamination with HIV infected blood.
PATHOGENESIS OF HIV
Selective tropism for CD4 molecule receptor
Internalisation
Uncoating and viral DNA formation.
Viral integration Viral replication. Latent period and immune attack. CD4+ T cell destruction. Viral dissemination. Impact of HIV infection on other immune cells. HIV infection of nervous system Clinical manifestations of HIV/AIDS.
Wasting Syndrom
Latent period and immune attack. CD4+ T cell destruction. Viral dissemination. Impact of HIV infection on other immune cells. HIV infection of nervous system Clinical manifestations of HIV/AIDS.
Wasting Syndrom
Viral dissemination. Impact of HIV infection on other immune cells. HIV infection of nervous system Clinical manifestations of HIV/AIDS.
Wasting Syndrom
HIV infection of nervous system Clinical manifestations of HIV/AIDS.
Wasting Syndrom
Declining immune function is wasting syndrome defined as ‘involuntary loss of body weight by more than 10%’. It occurs due to multiple factors such as malnutrition, increased metabolic rate, malabsorption, anorexia, and ill-effects of multiple opportunistic infections.
Persistent generalised lymphadenopathy.
PGL is defined as presence of enlarged lymph nodes >1 cm at two or more extrainguinal sites for >3 months without an obvious cause.
GI lesions and manifestations
Almost all patients with HIV infection develop gastrointestinal manifestations. These include: chronic watery or bloody diarrhoea, oral, oropharyngeal and oesophageal candidiasis, anorexia, nausea, vomiting, mucosal ulcers, abdominal pain.
Pulmonary lesions and manifestations.
These features are largely due to opportunistic infections causing pneumonia e.g. with Pneumocystis carinii, M. tuberculosis, CMV, Histoplasma, and Staphylococci.
Haematologic lesions and manifestations.
Mucocutaneous manifestations are allergic (e.g. drug reaction, seborrhoeic dermatitis), infectious (viral infections such as herpes, varicella zoster, EB virus, HPV;bacterial infections such as M. avium, Staph. aureus; fungal infections such as Candida, Cryptococcus, Histoplasma) and neoplastic (e.g. Kaposi’s sarcoma, squamous cell carcinoma, basal cell carcinoma, cutaneous lymphoma).
CNS lesions and manifestations.
These may be inflammatory, demyelinating and degenerative conditions. HIV encephalopathy or AIDSassociated dementia complex, is an AIDS defining condition and manifests clinically with deteriorating cognitive symptoms.
Gynaecologic lesions and manifestations.
s. Gynaecologic symptoms are due to monilial (candidal) vaginitis, cervical dysplasia, carcinoma cervix, and pelvic inflammatory disease.
Renal lesions and manifestations
Features of renal impairment may appear due to HIV-associated nephropathy and genitourinary tract infections including pyelonephritis.
Hepatobiliary lesions and manifestations.
. Manifestations of hepatobiliary tract are due to development of coinfection with hepatitis B or C, due to occurrence of other infections and due to drug-induced hepatic injury.
Cardiovascular lesions and manifestations.
Heart disease is common autopsy finding and include a form of dilated cardiomyopathy called HIV-associated cardio myopathy, pericardial effusion in advanced disease as a reaction to opportunistic infection, lymphoma and Kaposi’s sarcoma
Ophthalmic lesions
HIV associated ocular manifestations occur from opportunistic infections (e.g. CMV retinitis), HIV retinopathy, and secondary tumours.
Musculoskeletal lesions
These include osteoporosis, osteopaenia, septic arthritis, osteomyelitis and polymyositis.
Endocrine lesions
There is syndrome of lipodystrophy (buffalo hump) due to dyslipidaemia, hyperinsulinaemia and hyperglycaemia.
DIAGNOSIS OF HIV/AIDS
1. Tests for establishing HIV infection:
Antibody tests :ELISA. ,Western blot
Direct detection of HIV : p24 antigen capture assay,HIV RNA assay methods by reverse transcriptase (RT) PCR, branched DNA, nucleic acid sequence-based amplification (NucliSens),DNA-PCR by amplification of proviral DNA, Culture of HIV from blood monocytes and CD4+ T cells.
2. Tests for defects in immunity:CD4+ T cell counts.
- Rise in CD8+ T cells.
- Reversal of CD4+ to CD8+ T cell ratio.
- Lymphopenia.
- Polyclonal hypergammaglobulinaemia.
- Increased β-2 microglobulin levels.
- Platelet count revealing thrombocytopenia.
3. Tests for detection of opportunistic infections and
secondary tumours:
CD4+ T cell counts.
Diagnosis of organs involved in opportunistic infection and specific tumours secondary to HIV/AIDS is made by aspiration or biopsy methods.