
Multiple sclerosis
Table of Contents
What is Multiple Sclerosis?
Multiple sclerosis (MS) is an autoimmune inflammatory neurological condition. It destroys myelinated axons of the central nervous system (CNS) which affect the brain and the spinal cord . Causes long-term disability in adults.
What are the causes of Multiple sclerosis (MS)?
There are many researchers still finding the cause of MS but still does not understand. Some research shows genetic, viral infection, any kind of emotional trauma, or external environmental condition.
Incidence Rate of MS
In the UK, where the prevalence is approximately 120 per 100 000. The annual incidence is around 7 per 100 000, while the lifetime risk of developing Multiple sclerosis (MS) is about 1 in 400. The incidence of MS is higher in Northern Europeans and the disease is about twice as common in females.
What symptoms shown in Multiple Sclerosis(MS) ?
The Symptoms and signs of MS usually evolve over days or weeks, resolving over weeks or months.
- Patient with Multiple Sclerosis (MS) shows evidence of previous optic neuritis may be found in the form of an afferent pupillary deficit.
- In the last stage of the disease Intellectual impairment appears, Impairment of memory is common when there is a loss of frontal lobe functions.
- Relapsing/remitting sensory symptoms such as 1–2 relapses every
2 years, although this may decline with time. - Subacute painless spinal cord lesion
- Acute brainstem syndrome
- Subacute loss of function of upper limb (dorsal column deficit)
- 6th cranial nerve palsy
- Postural tremor
- Recurrent facial palsy( weakness of the facial muscles, )
- Trigeminal neuralgia( pain is caused by irritation of the trigeminal nerve )
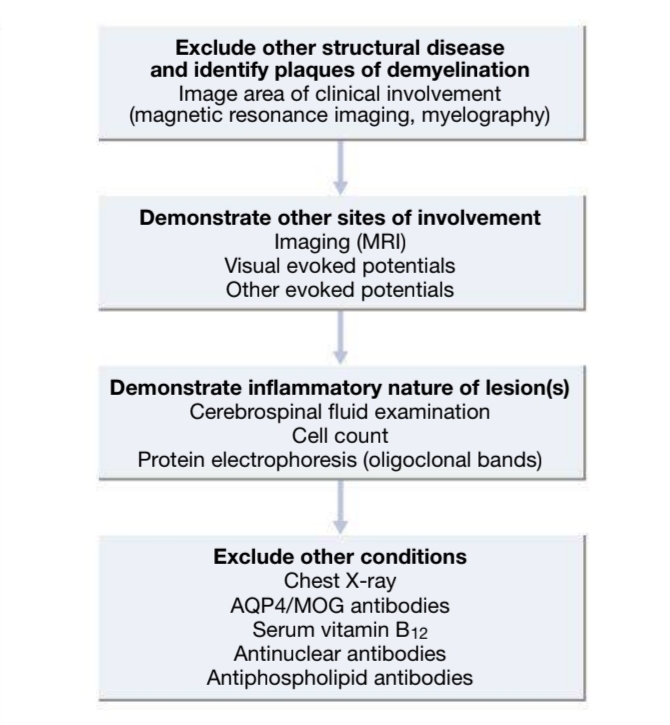
How to diagnose MS ?
There is no single diagnostic test that is done for MS and the results of the investigation needed to combined with the clinical picture to make a diagnosis such as
- MRI is the most important investigation
- Evoked potentials (visual, auditory or somatosensory) may detect clinically silent lesions.
What are the treatment options available?
The four different stages of treatment of Multiple sclerosis (MS) are, treatment of the acute episode, prevention of future relapses, treatment
of complications, and management of the patient’s disability.
The acute episode
In a disabling exacerbation of MS, pulses of high-dose glucocorticoid, given either intravenously or orally over 3–5 days,
will shorten the duration of the acute episode.
Disease-modifying treatment
The introduction of disease-modifying treatments (DMTs) for Multiple sclerosis (MS) initially, beta-interferons and glatiramer acetate. These drugs – are available orally. Careful selection and counseling of patients are necessary and these drugs should be supervised by teams experienced in their use, as recommended in national guidelines.
Clinical trials suggest that DMT options for primary and secondary progressive MS will be available in the coming years. Clinical trials involving stem cells are ongoing. Special diets, including gluten-free regimens or linoleic acid supplements, and hyperbaric oxygen therapy are popular with patients but their efficacy has not been demonstrated.
Multiple sclerosis in pregnancy
• Counselling: The provision of pre-conception counseling is best practice.
• Relapse risk: The effect of endocrine on the immune system ensure that the risk of relapse drops during pregnancy.
• Disease-modifying drugs: risk of teratogenicity means that all disease-modifying drugs should ideally be stopped 6–8 weeks before conception and recommenced after breastfeeding has stopped.
• Post-partum relapse rate: There is a high risk of relapse in the first year after delivery due to a rebound of immune system activity.
Complications in MS
- Spasticity
- Dysesthesia
- Fatigue
- Erectile dysfunction
Treatment for spastic patient can be physiotherapy , Baclofen (usually oral) ,Dantrolene ,Gabapentin , Sativex etc . If he /she is suffering for dysesthesia then take Carbamazepine, Gabapentin ,Phenytoin ,Amitriptyline.
Summary of Article
It is important to provide patients with Multiple sclerosis a careful explanation of the nature of the disease and its outcome. When and if disability occurs, the patients and their relatives need appropriate support. Specialist nurses working in a multidisciplinary team of health-care professionals are of great value in managing the chronic phase of the disease. Periods of physiotherapy and occupational therapy may improve functional capacity in those who become disabled, and guidance can be provided on the provision of aids at home, reducing handicap. Bladder care is particularly important.
Urgency and frequency can be treated pharmacologically but this may lead to a degree of retention with an attendant risk of infection. Urinary retention can be managed initially by intermittent urinary catheterization (performed by the patient, if possible) but an in-dwelling catheter may become necessary. Sexual dysfunction is a frequent source of distress. Sildenafil or tadalafil helps impotence in men, and skilled counselling and prosthetic aids may be beneficial. Pregnancy does not increase the risk of progression of MS but relapses may occur post-partum.
Recent Post