
How to perform Neurological assessment ?
-
 Dr.
Arpita Biswas
Dr.
Arpita Biswas
- Dr.Rahul Kr. Jha
- Disclaimer

Every Neurological assessment starts with taking the demographic data from patient. A demographic data is the personal information of patient like Name, Age, Gender, Address, Occupation, Date of Admission, and Date of Assessment, Referral From etc.
Demographic data is done when the patient is sitting in front of you. Whereas every Neurological assessment start as soon as the patient enter the consultation room .Before taking history of the patient, you can quickly observe:
- Level of consciousness
- Facial asymmetry
- Speech clarity (slurred speech?)
- Breathing difficulty
- Gait/balance (if they walked in)
In every neuro assessment, this helps you identify emergency signs like stroke, seizure, acute weakness etc.
Chief Complain
After you take data in neuro assessment, you start asking about the chief complain. The Problem facing by the patient written in patient language is chief complain. Ask them
- “What problem brings you here today?”
- “Can you describe your main complaint in your own words?”
- “When did this problem start?”
- “Was the onset sudden or gradual?”
- “Has the problem been continuous or does it come and go?”
Write the information in neurological assessment sheet as,
- Patient complains of _______________________ for _______ duration.
- Associated symptoms: __________________________________________.
- Functional limitations: (difficulty walking, speaking, weakness, imbalance, etc.)
History of Present illness
“Simply knowing the illness — for example, a patient saying ‘I have pain in my left shoulder’ — is not enough for proper clinical understanding. To assess the condition accurately, we must take a detailed History of Present Illness.
For instance, when a patient reports left shoulder pain, the neurological assessment HOPI allows us to find out:
- When the pain first appeared (hours, days, or months ago)
- How it began (after an injury, gradually over time, or without any clear cause)
- What the pain feels like (sharp, dull, throbbing, or radiating)
- Whether it is continuous or comes and goes
- Factors that worsen it (lifting the arm, sleeping on that side, working)
- Factors that reduce it (rest, medication, heat application)
- Any additional symptoms (numbness, tingling, weakness)
- How it affects daily tasks (difficulty combing hair, reaching overhead, dressing, or lifting objects).
The chief complaint tells us only the main problem, but the History of Present Illness gives the complete story behind the problem. This deeper understanding is essential part of neuro assessment for correct diagnosis, planning treatment, and guiding physiotherapy.
These Information are written in neurological assessment as
- Onset: Sudden / Gradual
- Duration: Since ______
- Progression: Improving / Worsening / Intermittent
- Location: Limb, side of body, face, etc.
- Character of symptoms:
- Weakness
- Numbness
- Tingling
- Loss of balance
- Visual disturbance
- Speech difficulty
- Headache
- Seizure
- Loss of consciousness
- Involuntary movements
- Aggravating factors: ____________
- Relieving factors: ______________
- Previous episodes: Yes/No – details.
- Effect on ADLs: Walking, dressing, eating, working, etc.
In every neurological assessment history also include Past Medical History, past surgical History, Family History etc.
Examination
Mneumonics
“My Cranial Motor Sensory Reflexes Got Assessed”
- Mental Status
- Cranial Nerves
- Motor System
- Sensory System
- Reflexes
- Gait
- Autonomic
Mental Status Examination (MSE)
This part of neuro assessment evaluates the patient’s cognitive abilities and overall mental functioning.
Key Areas to Assess
- Level of consciousness: Whether the patient is alert, drowsy, in stupor, or unconscious.
- Orientation: Ability to recognize person, place, and time.
- Memory: Test immediate recall, recent memory, and long-term memory.
- Speech and language: Observe clarity, fluency, and ability to comprehend and express.
- Mood and behavior: Note if the patient appears calm, anxious, irritable, or confused.
- Higher mental functions: Assess attention span, simple calculations (like serial 7s), and abstract reasoning.
Cranial Nerve Examination (I–XII)
Each cranial nerve has specific functions that should be tested.
- CN I – Olfactory Check the patient’s ability to identify different smells.
- CN II – Optic Assess visual acuity, peripheral fields, and perform a fundoscopic exam.
- CN III, IV, VI – Oculomotor, Trochlear, Abducens
Evaluate eye movements, pupil reaction to light, and look for drooping of eyelids. - CN V – Trigeminal
Test facial sensations, corneal reflex, and strength of chewing muscles. - CN VII – Facial
Observe facial movements (smile, frown, puff cheeks) and test taste on the front two-thirds of the tongue. - CN VIII – Vestibulocochlear
Check hearing using tests like Rinne and Weber, and assess balance. - CN IX & X – Glossopharyngeal and Vagus
Look for palate elevation, swallowing ability, and gag reflex. - CN XI – Accessory
Assess strength of shoulder shrug and head rotation. - CN XII – Hypoglossal
Ask the patient to protrude the tongue and observe for deviation or weakness.
Motor System Examination
Inspection
- Look for muscle wasting, asymmetry, or involuntary flickering movements (fasciculations).
Muscle Tone
- Increased tone (spasticity) suggests an upper motor neuron issue.
- Decreased tone (flaccidity) indicates a lower motor neuron problem.
Muscle Strength
- Grade using the MRC/MMT scale (0–5).
Principles of MMT – Click Here to read more
- Test major muscle groups: shoulder, elbow, wrist, hip, knee, and ankle.
Coordination
These tests are used to evaluate coordination of patient neuro assessment such as:
- Finger-to-nose test
- Heel-to-shin test
- Rapid alternating movements to check for dysdiadochokinesia
Sensory System Examination
Sensory examination include superficial, deep, cortical neuro assessment examination.
Superficial Sensations
- Light touch
- Pinprick (pain)
- Temperature
Deep Sensations
- Position sense (proprioception)
- Vibration sense
Cortical Sensations
- Two-point discrimination
- Stereo gnosis (recognizing objects by touch)
- Graphesthesia (identifying numbers/letters traced on hand)
- Sensory localization
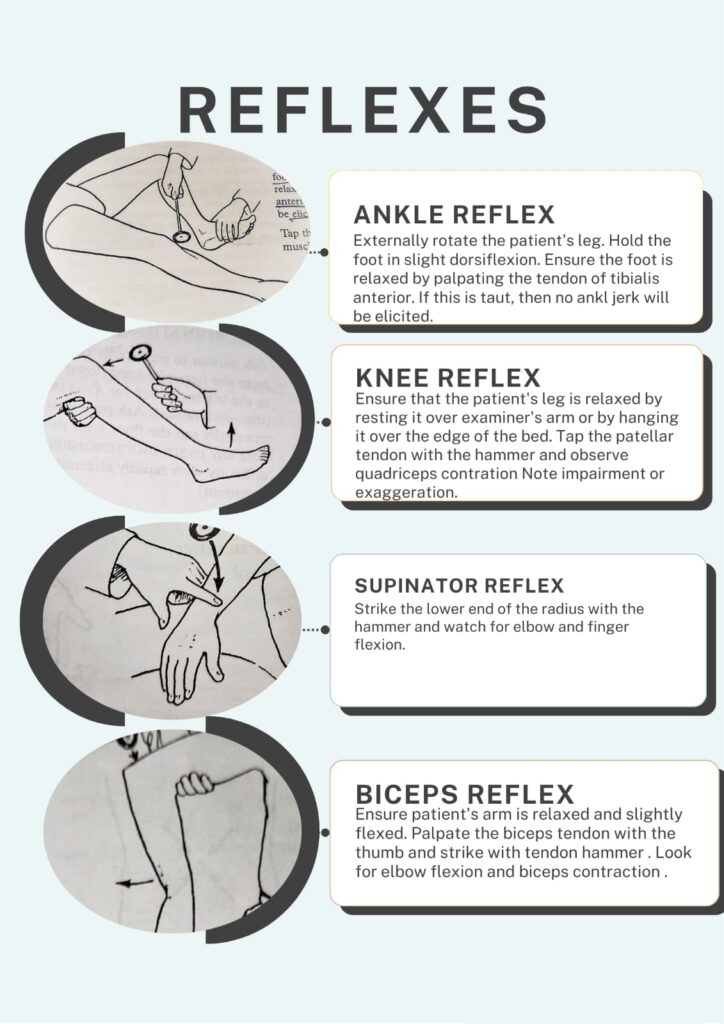
Reflex Testing
Deep Tendon Reflexes
- Biceps (C5)
- Brachio radialis (C6)
- Triceps (C7)
- Knee (L3–L4)
- Ankle (S1)
Reflex Grading Scale (0–4):
- 0: No reflex
- 2+: Normal response
- 4+: Very brisk or clonus
Superficial Reflexes
- Abdominal reflex
- Cremasteric reflex (in males)
Pathological Reflexes
- Babinski’s sign: Extension of big toe, indicates upper motor neuron involvement.



Gait and Balance Evaluation
When a therapist perform neurological assessment they start with observing the patient doing:
- Regular walking
- Walking on heels and toes
- Romberg test for balance
- Tandem walking (heel-to-toe)
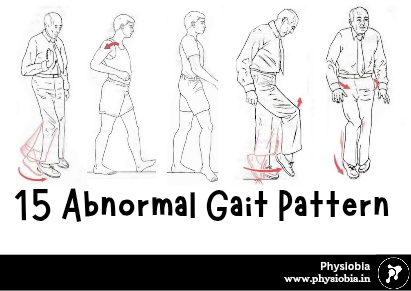
Identify gait patterns such as:
- Ataxic gait
- Parkinsonian gait
- Spastic gait
Top 15 abnormal gait pattern – Click Here to Read more



Autonomic Nervous System Assessment (when needed)
This includes checking:
- Blood pressure and heart rate variations
- Bowel and bladder functions
- Changes in sweating
- Pupillary reactions