
Top 15 Abnormal Gait Pattern
-
 Dr.
Arpita Biswas
Dr.
Arpita Biswas
- Dr.Rahul Kr. Jha
- Disclaimer

Table of Contents
Abnormal Gait
Gait is a medical term used for normal pattern of walking mechanism and Abnormal gait refers to the incorrect pattern of walking which is biomechanically wrong. This gait deviation can occur for three reasons. First, they may occur because of pathology or injury in the specific joint. Second, they may occur as compensations for injury or pathology in other joints on the same or ipsilateral side. Finally, they may occur as compensations for injury or pathology on the opposite or contralateral limb
Let’s understand some common types of abnormal gait
Antalgic (Painful) Gait
The antalgic or painful gait is self-protective and results from injury to the pelvis, hip, knee, ankle, or foot. The stance phase on the affected leg is shorter than that on the nonaffected leg because the patient attempts to remove weight from the affected leg as quickly as possible; therefore, the amount of time on each leg should be noted.
The swing phase of the uninvolved leg is decreased. The result is a shorter step length on the uninvolved side, decreased walking velocity, and reduced cadence. In addition, the painful region is often supported by one hand, if it is within reach, and the other arm, acting as a counterbalance, is outstretched. If a painful hip is causing the problem, the patient also shifts the body weight over the painful hip.
This shift decreases the pull of the abductor muscles, which reduces the pressure on the femoral head from more than two times the body weight to approximately body weight, owing to vertical instead of angular placement of the load over the hip.
Some Conditions that cause Antalgic Abnormal Gait
- Osteoarthritis – Common in the hip, knee, or ankle joints, causing pain with weight-bearing.
- Fractures – Stress fractures or traumatic fractures in the lower extremities.
- Tendinitis or Bursitis – Common in the trochanteric bursitis in the hip, prepatellar bursitis in the knee, or Achilles tendinitis in the ankle.
- Plantar Fasciitis – Heel pain causing avoidance of full weight-bearing
- Muscle Strains – Especially in the hamstrings, quadriceps, or calf muscles
- Ligament or Meniscus Injuries – Such as ACL tears or meniscal tears in the knee.
- Rheumatoid arthritis – Inflammatory joint disease leading to pain and stiffness in hip joint and knee joint
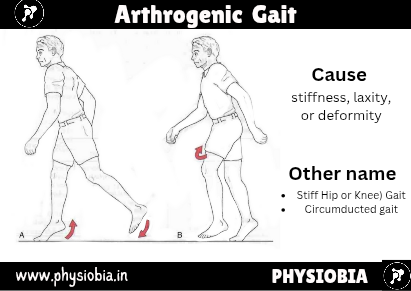
Arthrogenic (Stiff Hip or Knee) Gait
The arthrogenic gait results from stiffness, laxity, or deformity, and it may be painful or pain-free. If the knee or hip is fused or the knee has recently been removed from a cylinder cast, the pelvis must be elevated by exaggerated plantar flexion of the opposite ankle and circumduction of the stiff leg (circumducted gait) to provide toe clearance.
The patient with this gait lifts the entire leg higher than normal to clear the ground because of a stiff hip or knee. The arc of movement helps to decrease the elevation needed to clear the affected leg. Because of the loss of flexibility in the hip, knee, or both, the gait lengths are different for the two legs. When the stiff limb is bearing weight, the gait length is usually smaller.
To learn about the Muscle of the Thigh then Read Our Article – Muscles of the Thigh Region
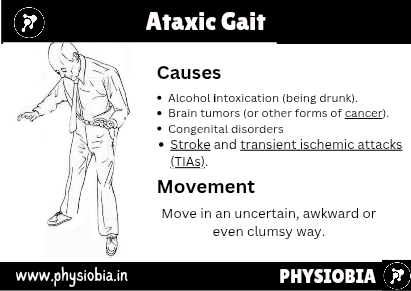
Ataxic Gait
If the patient has poor sensation or lacks muscle coordination, there is a tendency toward poor balance and a broad base. The gait of a person with cerebellar ataxia includes a lurch or stagger, and all movements are exaggerated. The feet of an individual with sensory ataxia slap the ground because they cannot be felt. The patient also watches the feet while walking. The resulting gait is irregular, jerky, and weaving. This is commonly found in Cerebral Palsy Patient
To learn about Types of Cerebral palsy and their specific Gait pattern Read Our Article –Cerebral palsy: 4 Types & its Cause
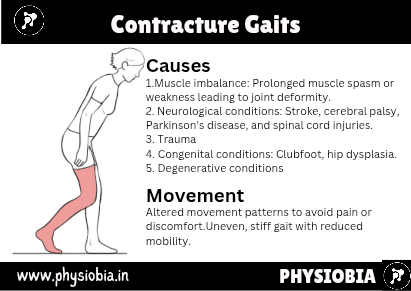
Contracture Gaits
If immobilization has been prolonged or pathology to the joint has not been properly cared for then the joints of the lower limb may exhibit contracture.
Hip flexion contracture often results in increased lumbar lordosis and extension of the trunk combined with knee flexion to get the foot on the ground.
With a knee flexion contracture, the patient demonstrates excessive ankle dorsiflexion from the late swing phase to the early stance phase on the uninvolved leg and early heel rise on the involved side in the terminal stance.
Plantar flexion contracture at the ankle results in knee hyperextension (midstance of affected leg) and forward bending of the trunk with hip flexion (midstance to terminal stance of affected leg). Heel rise on the affected leg also occurs earlier.



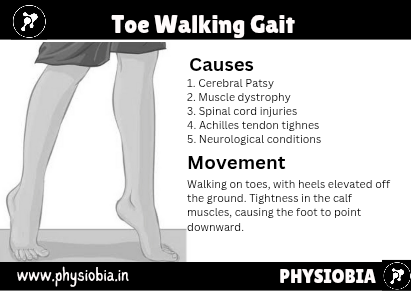
Equinus Gait (Toe Walking)
This childhood gait is seen with talipes equinovarus (club foot). Weight-bearing is primarily on the dorsolateral or lateral edge of the foot, depending on the degree of deformity. The weight-bearing phase on the affected limb is decreased, and a limp is present. The pelvis and femur are laterally rotated to partially compensate for tibial and foot medial rotation.
Learn about Clubfoot Deformity in Our Article – Foot deformity



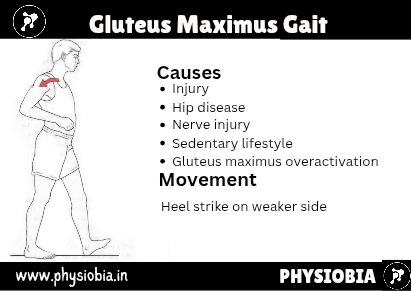
Gluteus Maximus Gait
If the gluteus maximus muscle, which is a primary hip extensor, is weak, the patient will make initial contact by heel called heel strike to maintain the hip extension of the stance leg. The resulting gait involves a characteristic backward lurch of the trunk.
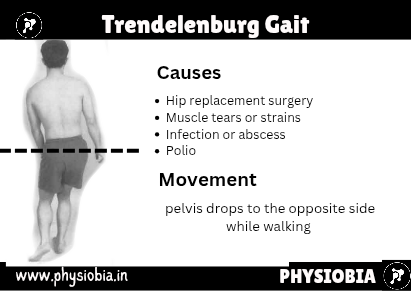
Gluteus Medius (Trendelenburg) Gait
If the hip abductor muscles (gluteus medius and minimus) are weak, the stabilizing effect of these muscles during the stance phase is lost, and the patient exhibits an excessive lateral list in which the thorax is thrust laterally to keep the center of gravity over the stance leg.
A positive Trendelenburg sign is also exhibited (i.e., the contralateral side droops because the ipsilateral hip abductors do not stabilize or prevent the droop). If there is bilateral weakness of the gluteus medius muscles, the gait shows accentuated side-to-side movement, resulting in a wobbling gait or “chorus girl swing.” This gait may also be seen in patients with congenital dislocation of the hip and coxa vara.



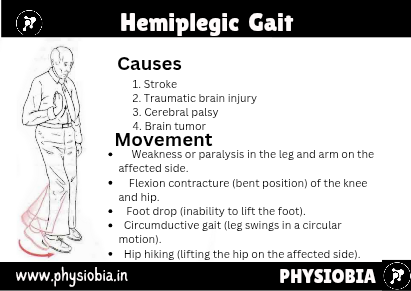
Hemiplegic or Hemiparetic Gait
The patient with hemiplegic or hemiparetic gait swings the paraplegic leg outward and ahead in a circle. ). In addition, the affected upper limb is carried across the trunk for balance. This is sometimes referred to as a neurogenic or flaccid gait.
Recent Studies show that post-stroke hemiplegic gait impairments as mechanical consequences of altered neural control mechanisms of human gait due to damage to motor cortex .
See Article – Post-stroke Hemiplegic Gait: New Perspective and Insights
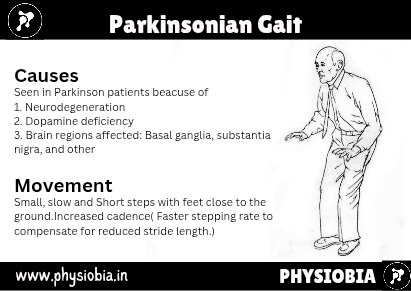
Parkinsonian Gait
The neck, trunk, and knees of a patient with Parkinsonian gait are flexed. The gait is characterized by shuffling or short rapid steps ( marche à petits pas) at times. The arms are held stiffly and do not have their normal associative movement.
During the gait, the patient may lean forward and walk progressively faster as though unable to stop (festination).
Plantar Flexor Gait
If the plantar flexor muscles are unable to perform their function, ankle and knee stability are greatly affected. Loss of the plantar flexors results in decrease or absence of push-off. The stance phase is less, and there is a shorter step length on the unaffected side.

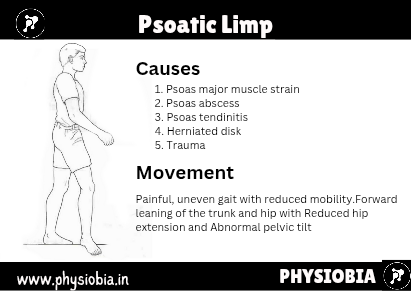
Psoatic Limp
The psoatic limp is seen in patients with conditions affecting the hip, such as Legg-Calvé-Perthes disease. The patient demonstrates a difficulty in swing-through, and the limp may be accompanied by exaggerated trunk and pelvic movement.
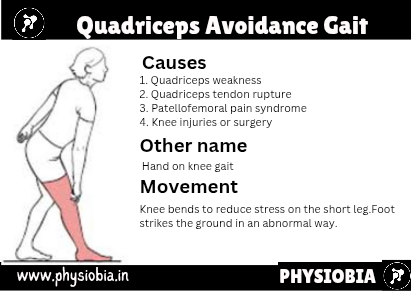
Quadriceps Avoidance Gait
If the quadriceps muscles have been injured (e.g., femoral nerve neuropathy, reflex inhibition, trauma—3°strain), the patient compensates in the trunk and lower leg. Forward flexion of the trunk combined with strong ankle plantar flexion causes the knee to extend (hyperextend).
The knee may be held extended by using the iliotibial band. If the trunk, hip flexors, and ankle muscles cannot perform this movement, the patient may use a hand to extend the knee.
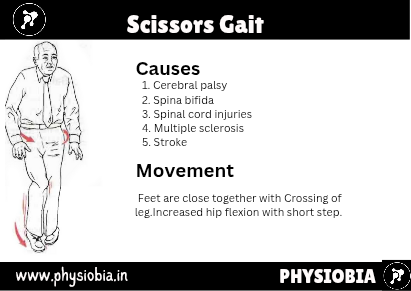
Scissors Gait
This gait is the result of spastic paralysis of the hip adductor muscles, which causes the knees to be drawn together so that the legs can be swung forward only with great effort. This is seen in spastic paraplegics and may be referred to as a neurogenic or spastic gait.
Short Leg Gait
If one leg is shorter than the other or there is a deformity in one of the bones of the leg, the patient may demonstrate a lateral shift to the affected side, and the pelvis tilts down on the affected side, creating a limp.
The patient may also supinate the foot on the affected side to try to “lengthen” the limb. The joints of the unaffected limb may demonstrate exaggerated flexion or hip hiking may occur during the swing phase to allow the foot to clear the ground.
The weight-bearing period may be the same for the two legs. How a patient adapts for leg length difference has wide variability. With proper footwear, the gait may appear normal. This gait may also be termed painless osteogenic gait.



Steppage or Drop Foot Gait
The patient with a steppage gait has weak or paralyzed dorsiflexor muscles, resulting in a drop foot. To compensate and avoid dragging the toes against the ground, the patient lifts the knee higher than normal.
At initial contact, the foot slaps on the ground because of loss of control of the dorsiflexor muscles resulting from injury to the muscles, their peripheral nerve supply, or the nerve roots supplying the muscles
SUBSCRIBE
subscribe to our newsletter and stay updated