
Rheumatic fever
Table of Contents
what is Rheumatic fever?
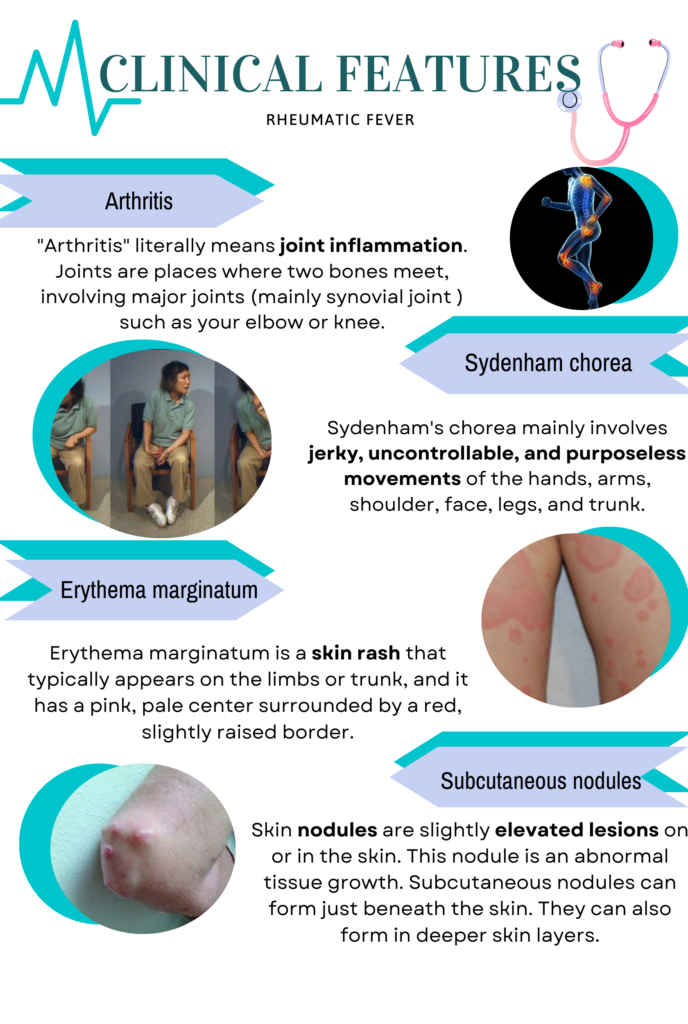
Rheumatic fever is an autoimmune and inflammatory disease that develops a complication of streptococcus infection such as strep throat or scarlet fever(caused by Group A-beta hemolytic streptococcus (GABHS) Rheumatic fever is manifested by: arthritis, carditis, chorea, erythema marginatum and subcutaneous nodules.
Pathophysiology Of Rheumatic fever.
The pathophysiology of ARF is characterized by aberrant immune response to GAS infection triggered by molecular mimicry between GAS antigens and self-antigens. This immune response typically manifests 2 to 4 weeks after initial GAS infection and may lead to the development of carditis, valvulitis, Sydenham chorea, subcutaneous nodules, erythema marginatum, and polyarthritis that is usually migratory. The severity and distribution of these manifestations vary significantly between individuals making diagnosis of ARF challenging. Early recognition of ARF using modified Jones criteria is essential in treating acute infection and preventing complications. A major long-term consequence is RHD, which carries the significant morbidity and mortality.
What are sign and symptoms of Rheumatic fever?
Symptoms of Rheumatic fever.
- Chest pain.
- Fatigue.
- Small, painless bumps beneath the skin.
- Flat or slightly raised, painless rash with ragged edge.
- Fever.
- Headache.
- Joint pain or swelling mostly in knees, ankles, elbows, and wrists. Joints may feel hot or tender.
- Pain in one joint that travels to another joints.
Signs of Rheumatic fever.
What things make Rheumatic fever worse?
Poverty and household overcrowding are associated with an increased prevalence of acute rheumatic fever and rheumatic heart disease, both of which remain public health problem in many low-income countries. Control efforts are hampered by scarcity of accurate data on disease burden, and effective approaches to diagnosis, treatment , and prevention.
How to diagnose Rheumatic fever?
1. Laboratory findings
In Rheumatic fever, the report shows High ESR, anemia, leukocytosis, and Elevated C- reactive protein. The ECG finding led to – a prolonged PR interval and Throat culture -GABH streptococci. The Echocardiogram report shows- valve edema, mitral regurgitation, LA &LV dilatation, pericardial, effusion, decreased
contractility.
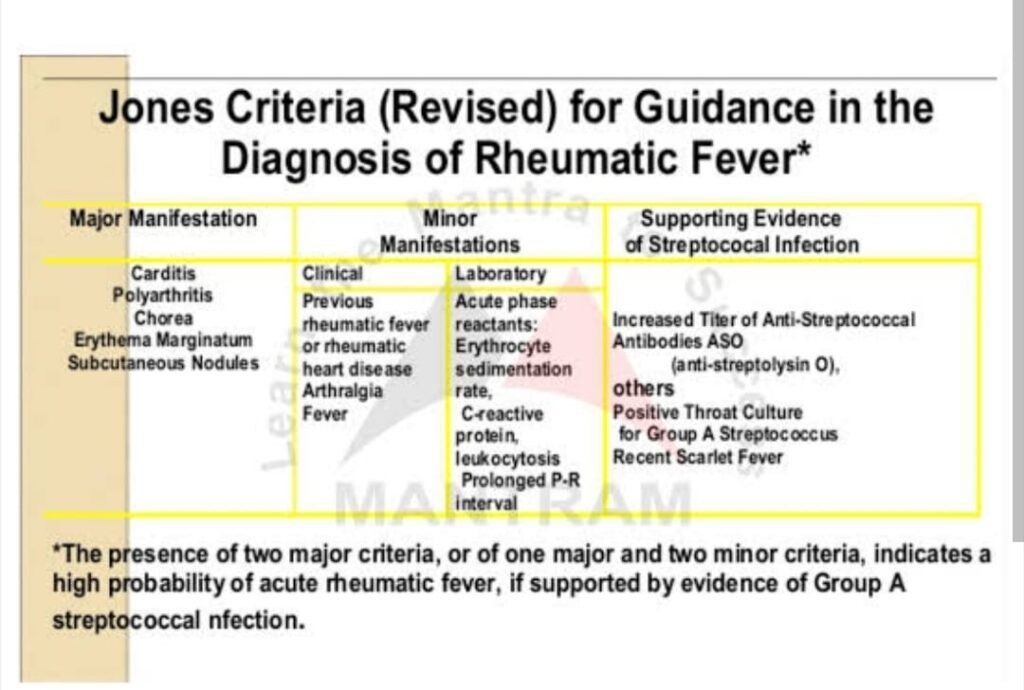
2. Modified John’s criteria
The Jones criteria is developed in 1944, then revised twice by American Heart Association (AHA), in 1992 and recently in 2015. According to American College of Cardiology revised John criteria (2015) says that :
Low-risk populations: The Major and minor criteria are as follows:
- Major criteria: carditis (clinical and/or subclinical), arthritis (polyarthritis), Erythema marginatum, chorea, and subcutaneous nodules.
- Minor criteria: polyarthralgia, fever (≥38.5° F), sedimentation rate ≥60 mm and/or C-reactive protein (CRP) ≥3.0 mg/dl, and prolonged PR interval (unless carditis is a major criterion).
High-risk populations: The Major and minor criteria are as follows:
- Major criteria: carditis (clinical and/or subclinical), Erythema marginatum, arthritis ( monopolyarthritis or polyarthritis, or polyarthralgia), chorea, and subcutaneous nodules
- Minor criteria: sedimentation rate ≥30 mm and/or CRP ≥3.0 mg/dl, fever (≥38.5° F), and prolonged PR interval (unless carditis is a major criterion).
Rheumatic Fever Treatment
Disclaimer ( Only For Educational purpose )
Step I : Primary prevention (eradication of streptococci)
Recommendations of the American Heart Association
| Agent | Dose | Mode/Duration |
|---|---|---|
| Benzathine penicillin G | 600000 U for patients 27 kg (60lb ) | Intramuscular |
| Penicillin V | Children : 250 mg 2-3 times daily Adolescent and adult : 500mg 2-3 times daily | Oral /10 d |
| For individuals allergic to penicillin Erythromycin : | 20-40mg /kg /d 2-4 times daily | Oral /10d |
Step II: Anti-inflammatory treatment
| Arthritis | Aspirin : 75 – 100 mg / kg / day dose for 6 weeks |
|---|---|
| Carditis | Prednisolone : 2-2.5 mg/kg/day, give as two divided doses for 2 weeks |
Step III: Supportive management & management of complications
- Bed rest
- Treatment of congestive cardiac failure: diuretics
- Treatment of chorea: diazepam Or haloperidol
- Rest to joints & supportive splinting
Step IV: Secondary prevention of Rheumatic fever
For individuals allergic to penicillin and sulfadiazine
| Erythromycin | 250 mg twice daily | Oral |
|---|
Complication Of Rheumatic Fever.
1. Rheumatic heart disease
Rheumatic Fever the most serious complication, occurs in 30% to 45% of Rheumatic Fever patients and leads to chronic rheumatic heart disease (RHD), which is characterized by progressive and permanent valvular lesions. RHD, which occurs 10 to 20 years after the original illness and is due to valvular damage by severe or recurrent bouts of Acute renal failure.
2. Associated other diseases
RHD can lead to the heart failure, pulmonary hypertension, dysrhythmias, embolic strokes, and sudden cardiac death.
3. Jaccuod arthropathy
Another complication of Rheumatic fever of Acute renal failure is Jaccuod arthropathy. This chronic, benign arthropathy may result in joint deformities due to repeated bouts of arthritis caused by ARF.
4. Joint deformities
The various joint deformities seen in Rheumatic fever include thumb subluxation, ulnar deviation, hallux valgus, and swan neck and boutonniere deformities of the fingers.
5. Psychiatric symptoms
Rheumatic Fever has been related to increased psychiatric symptoms in some patients.
References
Revised Jones Criteria for Acute Rheumatic Fever. American college of cardiology.
Acute Rheumatic Fever by MD Sadakat Chowdhury; Christian A. Koziatek; Michael Rajnik. PubMed
Revised johnes criteria for rheumatic fever. Image from Research gate