
Cranial Nerve
Table of Contents
What is Cranial Nerve ?
The cranial nerves are the 12 nerves in pairs that originate from the back of the Cranial bone and supply to muscles of eyeball, face, palate, pharynx, larynx, Tongue, and two larger muscles of neck, lung, heart, and most of the part of the gastrointestinal tract. Besides these, they are afferent to special senses like smell, sight, hearing, taste, and touch.
The Cranial nerve is in pairs and originates from the back of the brain for both left and right in the brain and body. For example, Optic nerves are in pairs, one nerve goes to the left eye and the other to the right eye.

What is the Name of the cranial nerve?
Features
There are 12 Cranial nerves. Each Cranial nerve has a number and a name as follows:
I – Olfactory
II – Optic
III – Oculomotor
IV – Trochlear
V – Trigeminal
VI – Abducent
VII – Facial
VIII – Vestibulocochlear
IX – Glossopharyngeal
X – Vagus
XI – Accessory
XII – Hypoglossal
Attachment of the nerve to the brain:
I, II to the forebrain
III, IV to the midbrain
V, VI, VII, VIII to the Pons
IX, X, XI, XII to the medulla oblongata
What is the role of the cranial nerve?
The Cranial Nerve plays a crucial role in controlling and coordinating all bodily sensory and motor functions.
Sensory nerve work in:
- Touch
- Hear
- See
- Smell
- Taste
Motor nerve work in:
Facial muscles and glands are innervated by nerves. Some cranial nerve work is both motor and sensory cranial nerve.
Mnemonic
According to BD Chaurasia’s Human Anatomy textbook, volume 4 in chapter 4 (Cranial Nerve ) gives the best mnemonic for remembering cranial nerves,
“oh, oh, oh, try, try, again a failure, victory give value and happiness”
Olfactory Cranial nerve
The Olfactory Cranial nerve is an Olfactory smell pathway made up of olfactory cells (16-20 million in man) are bipolar neurons. They lie in an olfactory part of the nasal mucosa and serve both as receptors as well as the first neurons in the olfactory pathway. It is the First cranial nerve in 12 pairs of cranial groups.
There is an olfactory nerve, about 20 in number, representing the central processes of the olfactory cells.
Damage to Olfactory nerve
When there is damage to the olfactory Cranial nerve leads to various clinical anatomical diseases such as:
Anosmia: Loss of olfactory fibers with aging.
Allergic rhinitis: causes temporary olfactory impairment.
Head injury: CSF rhinorrhea that is CSF leakage through the nose.
Meningioma: The anterior cranial fossa may press on the olfactory bulb or olfactory tract resulting in Anosmia.
Uncinate fits: Lesion of the lateral olfactory area may cause temporal lobe epilepsy or uncinate fits. These fits are of imaginary disagreeable odors with the involvement of tongue and lips.
In complete paralysis of the tongue. Protrusion of the tongue is not possible. Speech and swallowing are affected taste and touch sensations are normal.
Optic Cranial nerve
The Optic Cranial nerve is the second cranial nerve in the Optic visual pathway. Human vision is binocular, though one sees with both eyes, the inverted images formed are seen as one and straight only. Human vision is stereoscopic, i.e. one sees.
Height, width, and thickness of the object. Human vision is colored, one sees different colors put up by nature. When one looks at an object; both eyes are focused on it. The right eye sees a little additional of the right side whereas the left eye sees a little additional of the left side of the object. These visions are monocular. The main part is binocular vision.
These are (1)” Pupillary light reflex (2) Accommodation reflex (3) Dilation of the pupil (4) Corneal /Conjunction reflex, and (5) visual body reflex”.
Damage to Optic nerve
Papilloedema: Results of increased intracranial pressure. It leads to swelling of the optic disc due to blockage of tributaries of the retinal veins.
Optic neuritis: Lesion of the optic nerve that results in a decrease in visual acuity. The optic disc appears pale and smaller.
Foster Kennedy syndrome: A tumor at the base of the frontal lobe resulting in compression of the nerve.
Argyll Robertson pupil: In this condition. The accommodation reflex is present but the light reflex is absent. The Pretectal area is affected.
Oculomotor Cranial Nerve
The Oculomotor Cranial Nerve is the third cranial nerve distributed to the extraocular as well as the intraocular muscle. Since it is a somatic motor nerve, it is in series with IV, VI, and XII cranial nerve, and also with the ventral root of the spinal nerve.
The function of this nerve help in the movement of eyeball muscle and contraction of the pupil and accommodation.
Damage to Oculomotor nerve
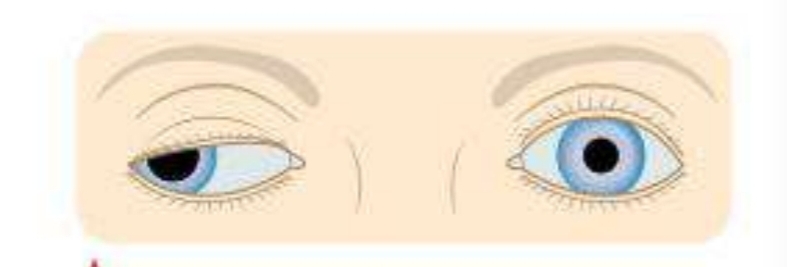
Complete and total paralysis of the third nerve results in:
- Ptosis, i.e. drooping of the upper eyelid.
- Lateral spuint
- Dilatation of the pupil
- Loss of accommodation due to the paralysis of ciliary muscle.
- Slight Proptosis, i.e. Forward projection of the eye.
- Diplopia or double vision.
- Weber’s Syndrome
Trochlear Cranial Nerve
The Trochlear Cranial Nerve supplies only the superior oblique muscle of the eyeball. It is the only cranial nerve that emerges on the dorsal aspect of the brain stem. The function of this nerve help in the lateral movement of the eyeball and transfer proprioceptive impulses from the muscle to the mesencephalic nucleus of the V nerve.
Damage to Trochlear nerve
When the Trochlear nerve is damaged, diplopia occurs on looking downwards; vision is single so long as the eyes look above the horizontal plane. Paralysis of trochlear nerve results in defective depression of adducted eye.
Trigeminal Cranial Nerve
Trigeminal Cranial Nerve is the largest cranial nerve. It comprises three branches, two of which are purely sensory, and the third, the largest branch is mixed nerve. The trigeminal nerve is the nerve of the first brachial arch.
Three divisions of the trigeminal nerve are as follows:
- Ophthalmic, the first division carries sensory fibers from the structure derived from the Frontonasal process.
- Maxillary, the second division conveys afferent fibers from structures derived from the maxillary process.
- Mandibular, the third mixed division carries sensory fibers derived from the mandibular process.
Damage to Trigeminal nerve
Hypoacusis, i.e. partial deafness to low-pitched sounds due to paralysis of the tensor tympani muscle.
Trigeminal neuralgia: Pain along the distribution of the nerve which is caused due to local lesion or unknown cause.
Abducent Cranial Nerve
Abducent Cranial Nerve supplies the lateral rectus muscle of the eyeball. The function of this nerve help in the lateral movement of the eyeball and transfer proprioceptive impulses from the muscle to the mesencephalic nucleus of the V nerve.
Facial Cranial Nerve
The facial Cranial Nerve is a seventh cranial nerve that is responsible for the muscle facial expression and for the elevation of the hyoid bone. The fibers of the facial nerve are secretomotor to the sub-mandibular and sublingual salivary glands, the lacrimal gland, and glands of the nose, palate, and pharynx.
Damage to Facial Nerve
Bell’s palsy: Sudden paralysis of the facial nerve at the stylomastoid foramen, results in asymmetry of the corner of the mouth, inability to close the eye, the disappearance of the nasolabial fold, and loss of wrinkling of skin of the forehead on the same side.
Crocodile tears syndrome: Lacrimation during the eating occurs due to aberrant regeneration after trauma.
Ramsay –Hunt syndrome: Involvement of the geniculate ganglia by herpes zoster results in this syndrome. It shows following symptoms: Hyperacusis, Loss of Lacrimation, Loss of sensation of taste in the anterior two-thirds of the tongue, Belly’s palsy, and lack of salvation.
Vestibulaocochlear Cranial Nerve
The Vestibulocochlear Cranial Nerve is the Eighth cranial(VIII) nerve. The Nerve comprises hearing and vestibular parts. It belongs to special somatic afferent columns. It takes all the sensory information from the ear and coordinates the function of hearing and posture balance in the body.
They have two branches, a cochlear branch which works for hearing sensation, and a vestibular branch which works for balance, spatial sensation, and posture coordination. The anatomical view of the Vestibulocochlear Nerve passes through the internal acoustic meatus and goes to vestibular, cochlear nuclei, and Medulla oblongata
The vestibular nerve handles balance and equilibrium, while cochlear nerve is responsible for hearing.
Damage to Vestibulocochlear Nerve
If there is damage to the eighth cranial nerves due to some injury or infection can lead to some pathological conditions such as,
Deafness: There are three types of deafness.
- Conduction deafness
- Sensorineural deafness
- Cortical deafness
Vertigo: This is an illusion of rotatory movement due to the disturbed orientation of the body in space. The patient feels that the environment is moving.
Tinnitus: It is the sensation of buzzing, ringing, hissing, or singing quality.
Acoustic neuroma: It is a slow-growing tumor of neurolemmal cells. It causes an early loss of hearing.
Glossopharyngeal Cranial Nerve
The Glossopharyngeal Nerve is the ninth cranial nerve. It is a motor nerve to the stylopharyngeus. It is the secretomotor nerve to the parotoid gland and gustatory to the posterior one-third of the tongue including circumvallates papillae. It is sensory to the pharynx, the tonsil, the soft palate, the posterior one-third of the tongue, the carotid body, and the carotid sinus.
Damage to Glossopharyngeal Nerve
Glossopharyngeal neuralgia: It is short sharp severe pain in the tonsillar area of the pharynx.
Pharyngitis: It may cause referred pain in the ear as both are supplied by the IX nerve.
Jugular foramen syndrome: It is due to injury at jugular foremen resulting in multiple cranial nerve palsies.
Vagus Cranial Nerve
The Vagus nerve is the tenth cranial nerve. It is so called because of its extensive (‘vagus’)course through the head, the neck, the thorax, and the abdomen. The fibers of cranial root ofthe accessory nerve are also distributed through it.
Paralysis of the vagus nerve produces:
- Nasal regurgitation of swallowed liquids.
- Nasal Twang in voice
- Hoarseness of voice
- Flattening of the palatal arch
- Cadaveric position of vocal cord
- Dysphagia
Accessory Cranial Nerve
The accessory Nerve is the eleventh cranial nerve. It has two roots, cranial and spinal. The cranial root is a special visceral (branchial ) efferent. It arises from the lower part of the nucleus ambiguus. It is distributed through branches of the vagus to muscles of palate, the pharynx, the larynx, and possibly the heart.
The spinal root is also a special visceral efferent. It arises from a long spinal nucleus situated in the lateral part of an anterior grey column of the spinal cord extending between segments C1 to C5. It supplies the sternocleidomastoid and the trapezium muscles. Lesion of the spinal root of the accessory nerve causes drooping of the shoulder and inability to turn the chin to the opposite side.
Damage of Accessory Cranial Nerve
Spasmodic torticollis : Irritation of the nerve resulting in clonic spasm of the sternocleidomastoid and trapezius muscles.
Hypoglossal Cranial Nerve
Hypoglossal in the twelfth cranial nerve. It supplies the muscle of the tongue. The hypoglossal nerve is tested clinically by asking patient to protrude his/her tongue. Normally, the tongue protrudes straight forward. If nerve is paralyzed, the tongue deviates to paralyzed side.
Damage of Hypoglossal Cranial Nerve
Bilateral paralysis of XII nerves results
Related post
What is the best diet to lower LDL cholesterol?
What is the best diet to lower LDL cholesterol? Introduction If you are concerned about high cholesterol, especially elevated LDL (Low-Density Lipoprotein) cholesterol, making the
What is best diet for high cholesterol ?
What is best diet for high cholesterol ? Maintaining healthy cholesterol levels is essential for protecting the heart and reducing the risk of cardiovascular
Best 25 Heart Healthy Foods to Eat
Best 25 Heart Healthy Foods to Eat Heart disease remains one of the leading health concerns worldwide, but many risk factors can be managed through
Sharp Pain in the Heel of My Foot: Causes and Treatment
Sharp Pain in the Heel of My Foot: Causes and Treatment Pain in the heel of my foot is one of the most common foot
Why my heel hurts when i walk : Possible Reasons and Fixes
Why my heel hurts when i walk : Possible Reasons and Fixes Heel pain can make everyday activities difficult. Many people notice discomfort while getting

8 best pain killers for muscle pain
8 best pain killers for muscle pain Pain is one of the most common health complaints worldwide, and pain killers are often the first solution