What is pneumonia?
Pneumonia is an acute respiratory infection in which the air space filled with fluid leads to inflammation of the lungs.
“Consolidation ” (meaning solidification ) used for the gross and radiologic appearance of lungs
Sign & Symptom
Pneumonia, particularly lobar pneumonia such as fever, rigors, shivering and malaise, predominate, and delirium may be present. The loss of appetite and headache is frequently reported.
During pulmonary pneumonia symptoms include cough, which at first is characteristically short, painful and dry, but later is accompanied by the expectoration of mucopurulent sputum. Rust-colored sputum may be produced by patients with Strep. pneumonia infection.
Upper abdominal tenderness is sometimes seen in patients with lower lobe pneumonia.
When there is consolidated, the lung is typically dull to percussion and, as conduction of sound is enhanced, auscultation reveals bronchial breathing and whispering pectoriloquy; crackles are heard throughout the chest area of patient.
What are the ways pneumonia spreads?
- When any person inhales these microorganisms, directly enter to the body causing Pneumonia.
- When this inhalation of organisms enters to lower airways called aspiration
- The direct inhalation of infectious particles in the air where it directly extends from the upper airways and hematogenous spread.
- Direct spread (from the site of infection). When the infection spreads from person to person through cough, sneezing, or talking respiratory droplets into the air causing pneumonia.
Normal defense mechanism of lung’s
- Nasopharyngeal filtering action
- Muscociliary action of lower respiratory airways
- Presence of phagocytosing alveolar macrophages
- Immunoglobulin
When there is a failure in this defense mechanism leads to pneumonia such as Altered consciousness seen in Patient such as :
- Coma
- Trauma
- Seizures
- cerebrovascular accidents
- drugs overdose
- alcoholism
Mucociliary cells are damaged in people who are in :
- smoking
- old age
- viral infection
Depressed coughing seen during :
- old age
- weakness
- Obstructive pulmonary diseases
Macrophages are destroyed in a person who is :
- Smoking
- Hypoxia
- Starvation
Classification of Pneumonia
- Anatomic region
- Lobar Pneumonia
- Bronchopneumonia
- Intestitial pneumonia
- Clinical setting
- Community-acquired pneumonia ( outside )
- Healthcare-associated pneumonia ( inside the hospital )
- Ventilator-associated pneumonia
- Etiology { causes }
- Bacterial Pneumonia is caused by bacteria
- Viral Pneumonia is caused by a virus
- Pneumonia is caused by other causes.
How to diagnose pneumonia?
Blood test
Full blood count
• Very high (> 20 × 109 /L) or low (< 4 × 109 /L) white cell count: marker
of severity
• Neutrophil leucocytosis > 15 × 109 /L: suggests bacterial etiology.
• Haemolytic anemia: occasional complication of Mycoplasma
Urea and electrolytes test
• Urea > 7 mmol/L (~20 mg/dL): marker of severity
• Hyponatraemia: marker of severity
Liver function tests
• Abnormal if basal pneumonia inflames the liver
• Hypoalbuminemia: a marker of severity
Blood culture
• Bacteremia: a marker of severity
Cold agglutinins
• Positive in 50% of the patients with Mycoplasma
Arterial blood gases
• Measure when SaO2 < 93% or when clinical features are severe, to assess ventilatory failure or acidosis.
Sputum
Sputum samples
• culture ,Gram stain , and antimicrobial sensitivity
testing
Oropharynx swab
• Polymerase chain reaction for Mycoplasma pneumoniae and other atypical pathogens
Urine test
• Pneumococcal and/or Legionella antigen
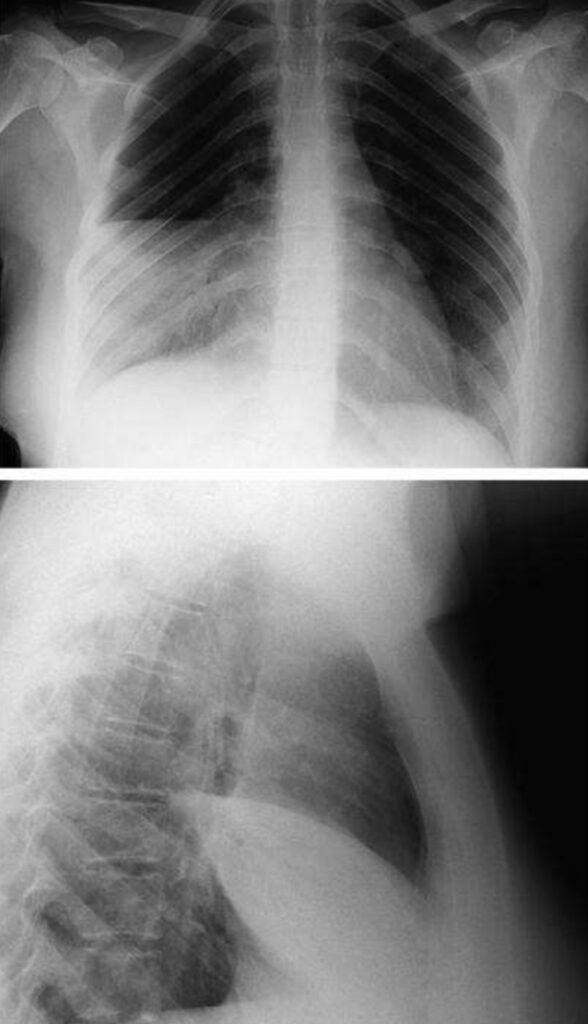
Lobar pneumonia
• Patchy opacification evolves into homogeneous consolidation of affected lobes
• Air bronchogram (air-filled bronchi appear lucent against consolidated lung tissue)
Bronchopneumonia
• Typically patchy and segmental shadowing.
• Para-pneumonic effusion, intrapulmonary abscess, or empyema Staphylococcus aureus
• Suggested by multilobar shadowing, cavitation, pneumatoceles and abscesses.
Pleural fluid
• Always aspirate and the culture when present in more than trivial
amounts, preferably with ultrasound guidance.
-