Proprioceptive Neuromuscular facilitation
Table of Contents
What is PNF?
The full form of PNF is Proprioceptive Neuromuscular facilitation. It is a stretching technique that helps to improve muscle elasticity and active and passive range of motion. Recent research shows that PNF increases AROM and PROM.
The techniques of PNF ( Proprioceptive Neuromuscular facilitation) mainly involve stimulating the proprioceptors to increase the demand on the neuromuscular mechanism to obtain and facilitate response. They are used for proprioceptive, cutaneous, and unitary input.
Neuromuscular = Nerve + muscle involvement
Facilitation = means making it easier
PNF was developed by Dr. Herman Kabat and Dr Margaret Knott between 1946 and 1951.
Basic Neurophysiological of PNF
Facilitation
An impulse causing the recruitment of motor neurons in the spinal cord which results in increased excitability in the muscle and weak muscles would aided through PNF facilitation.
Inhibition
Any stimulus that caused motor neurons to drop away from the discharge zone. Results in decreased excitability of motor neurons and muscle spasticity decreased.
Types of PNF
There are two major types of PNF, one is the contract-relax method (CR) and the other one is the contract-relax-antagonist-contract method (CRAC).
Contract-relax method (CR): This technique involves contracting, holding, relaxing, and stretching a muscle group. This method is also called the hold-relax method.
Contract-relax-antagonist-contract method (CRAC): This technique focuses on antagonistic muscle pairs. This method is also called hold -relax -contract method.
Neurological phenomena in PNF
The phenomena that make PNF an effective treatment and diagnostic tool for physiotherapists are :
- Reciprocal inhibition
According to this phenomenon the antagonist’s muscles are evoked by the contraction of the agonist’s muscle. Simply means when the agonist is activated antagonist is inactivated vica versa. PNF is a phenomenon in man and must be suspected of playing a major role in the control of voluntary movements.
- Autogenic inhibition
Autogenic inhibition is a phenomenon in which stretched muscle in the form of a decrease in excitability because of inhibitory signals sent from the GTOs of the same muscle which create tension within GTOs. PNF inhibits the muscle either through activation of GTO.
Goals of PNF
- PNF helps to increase strength, flexibility, coordination, and functional mobility.
- The main goal of PNF treatment is to facilitate the patient in achieving a movement or posture.
- PNF improves ADL’s functional mobility and athletic performance
- PNF is mainly used in orthopedic rehabilitation for musculoskeletal injuries and neurological rehabilitation.
- PNF can be used for any condition, however, the patient’s condition level may require modification.
How Can it Benefit you?
This article also explaine about PNF stretching benefits listed below,
- Increases ROM: Current evidence shows that the four theoretical mechanisms that effectively increase the range are autogenic inhibition, reciprocal inhibition, stress relaxation, and gate control theory. This effect of PNF is visible regardless of genders and age groups .
- Enhance muscle flexibility: There are studies which says that PNF help to enhance flexibility .Best useful for hamstring and calf .
- Enhance muscle strength: Muscular strenght can boost by PNF stretch when performed before less strenuous exercises( activity required more energy ).Best effective in tissue damage or received invasive surgeries.
- Increased muscle length: In stretch technique ,when the muscle is stretched beyond its active ROM and told to give resist .Slowly lead to increase in muscle and tendon length which ultimate results in production of greater amount of force because of the length-tension relationship.
- Enhance functional movements: The study shows that even in untrained individual can lead to enhancement of functional movement.
Technique of PNF
The basic principle of PNF includes these variables such as,
- Resistance
- Irradiation and reinforcement
- Manual contact
- Stretch
- Verbal commands
- Traction and approximation
- Timing
- Body positioning and body mechanics
The proper way to perform PNF with certain steps .These steps are as follows,
- Pattern of facilitation
- Mass movement patterns are used as the basis upon which all techniques of PNF are superimposed.
- The patterns of movement USED IN PNF are spiral and diagonal and they are closely allied to those of normal functional movement.
- This movement can be observed every day, for example, at work, during sports activities
- During PNF, the Components of movement are;
- Flexion /Extension
- Abduction /Adduction
- Rotatory
- Manual contact
Manual contact should be purposeful, directional, and comfortable.
- Stretch Effects
- Stimulates the activity of muscle spindle
- Any contraction of muscle on stretch will result in movement
- Traction
Traction is the elongation of trunks or extremities.
- Approximation uses
- Promote stabilization
- Facilitate weight bearing and contraction of postural muscle
- To resist some component of motion.Example – use of approximation at end of shoulder flexion to resist scapula elevation.
- Commands
- Louder command – stronger muscle contraction
- Softer and calmer tone – relaxation and relief of pain
- Maximal resistance
Opposing force to the patient’s movement is called maximal resistance
- Uses
- Facilitate the ability of muscles to contract
- Increases motor control and increase strength
- Help the patient gain awareness of motion
- Reinforcement
Reinforcement means ” to strengthen by fresh addition, making stronger “
PNF Stretching Techniques
PNF Stretching techniques require that patients has normal innervation and voluntary control of either the range – limiting target muscle or the muscle on the opposite side of the joint.As such, these techniques cannot be used effectively for patients with paralysis or spasticity resulting from neuromuscular disease or injury .
Types of PNF Stretching
There are several types of PNF stretching procedures ,all of which have been shown to improve ROM .They include:
- Hold-relax (HR)or contract -relax (CR)
- Agonist contraction (AC)
- Hold-relax with agonist contraction (HR-AC)
With classic PNF, these technique are always performed with combined muscle groups acting in diagonal patterns . Over time the techniques have been modified by clinicians and other to include stretching in a single plane or opposite the line of pull of a specific muscle group .
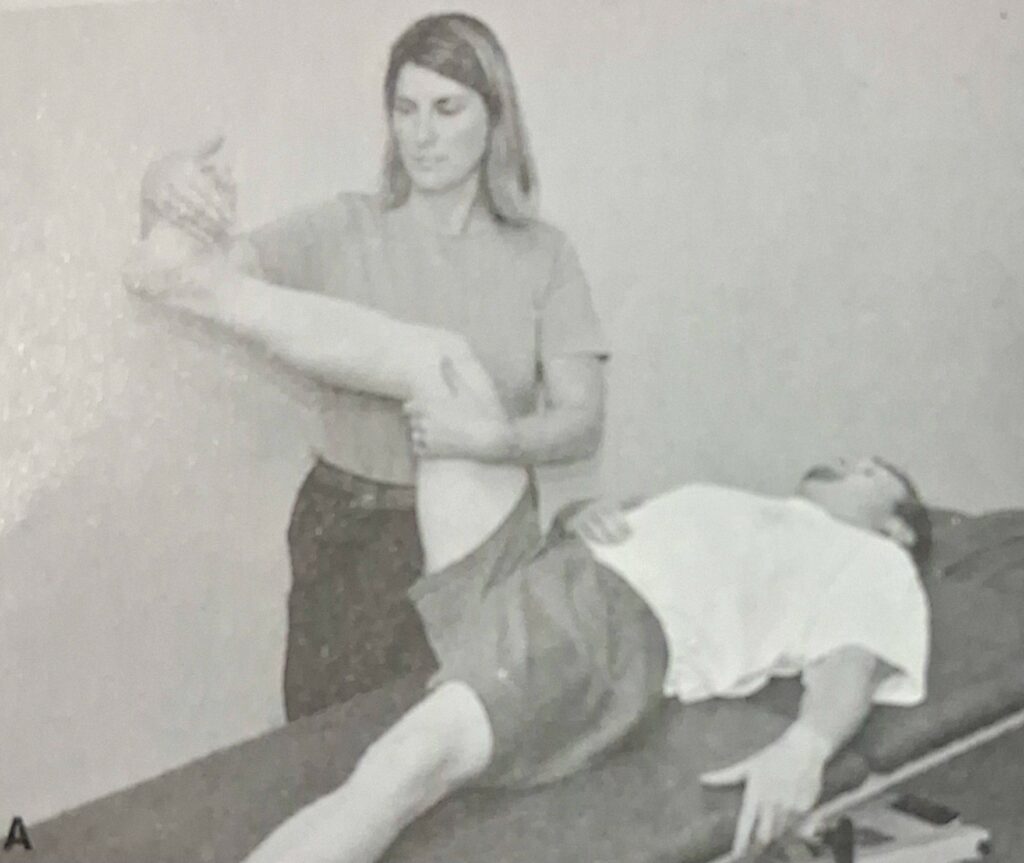
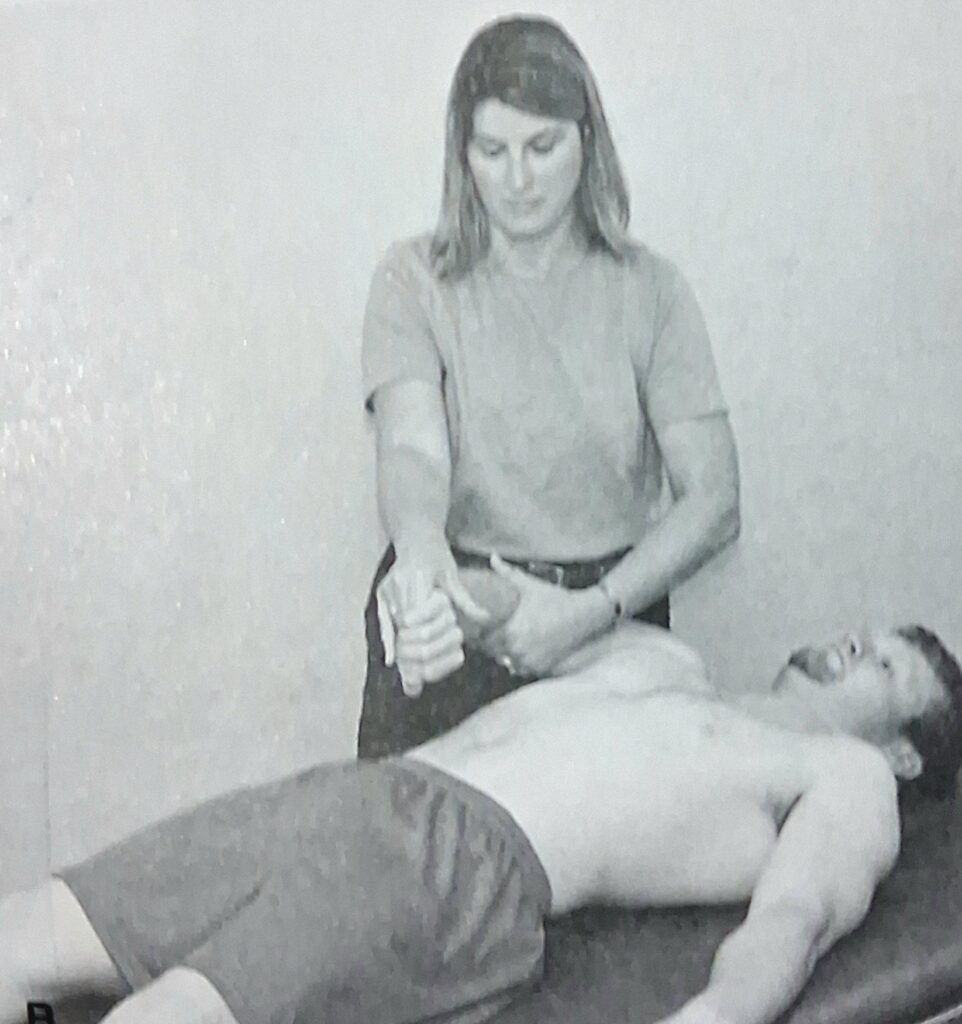
Upper limb PNF pattern
D1 Flexion
Starting position: Position the upper limb in shoulder extension, abduction and internal rotation, elbow extension, forearm pronation, and finger wrist and finger extension with the hand about 8 to 12 inches from the hip.
Hand placement: Place the index and middle finger of your left hand on the volar surface of the distal forearm or at the cubital fossa of elbow.
Verbal command: “Squeeze my finger turn your palm up; pull your arm up and across your face.
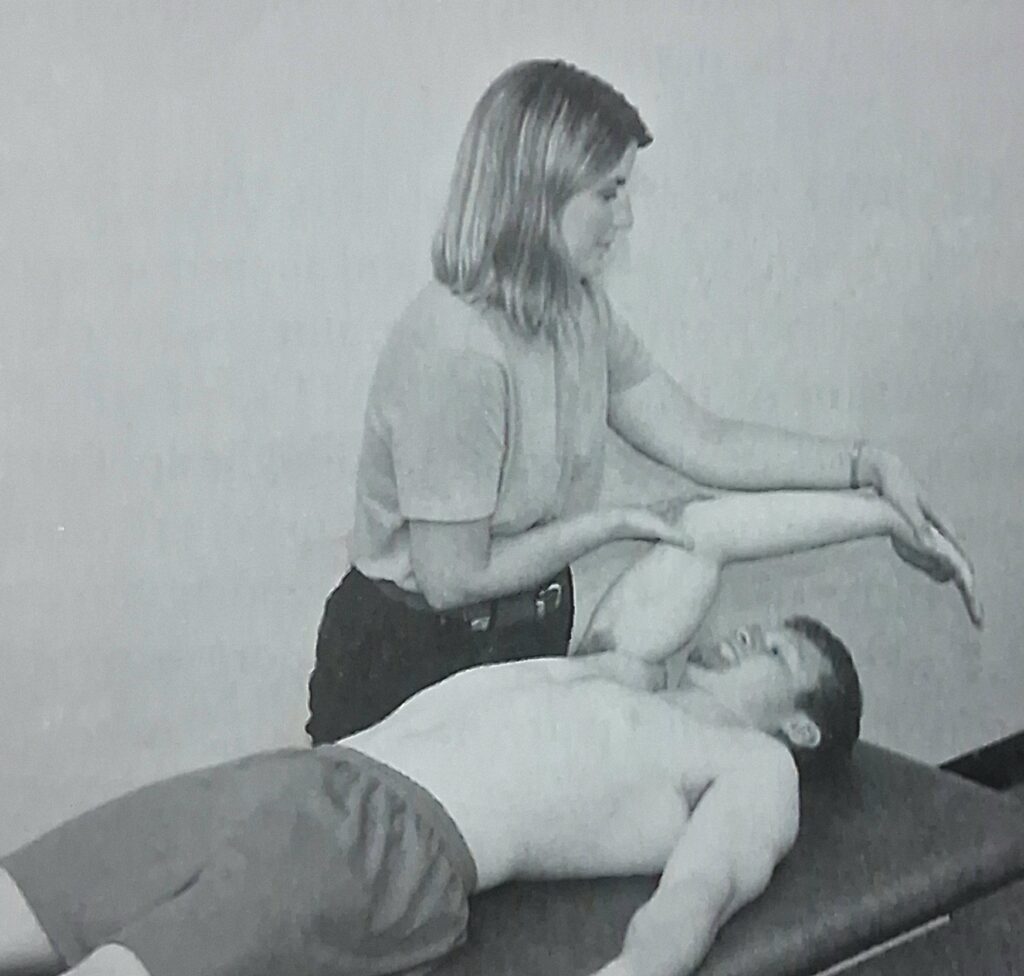
D1 Extension
Starting position: Similar to D1 Flexion in PNF pattern.
Hand placement: Grab the dorsal surface of the patient and finger with your right hand using a lumbrical grip. Place your left on the extensor surface of the arm just proximal to the elbow.
Verbal command:” Open your hand; Pull your arm down and out “
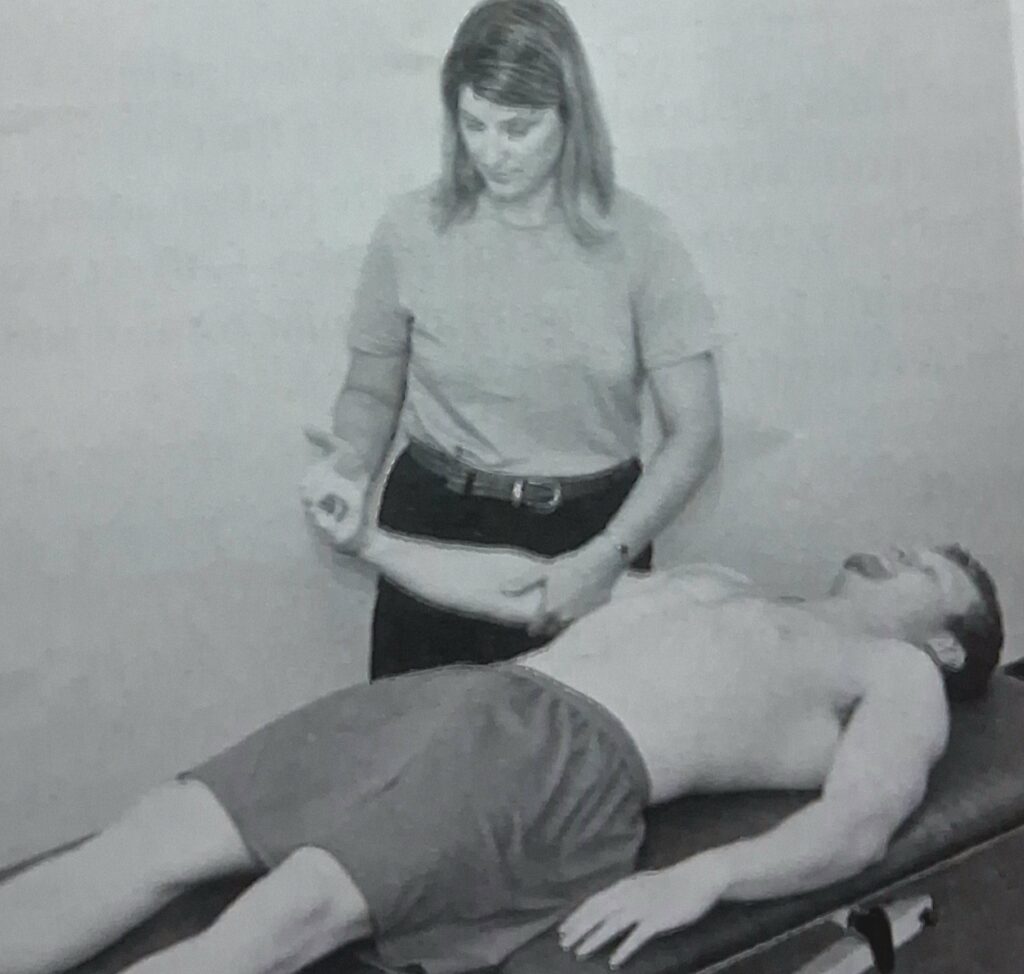
D2 Flexion
Starting Position: Position of upper limb in shoulder extension, adduction, and internal rotation; elbow extension, forearm pronation; and wrist and finger flexion. The forearm should lie across umbilicus.
Hand placement: Grasp the dorsum of the patient hand with your hand using a lumbrical grip. Grasp the dorsal surface of the patient’s forearm close to elbow with your right hand.
Verbal commands: As you apply a quick stretch to the wrist and finger extensors, tell the patients . “Open your hand and turn it to your face”,” Lift your arm up and out, “Point your thumb out “.
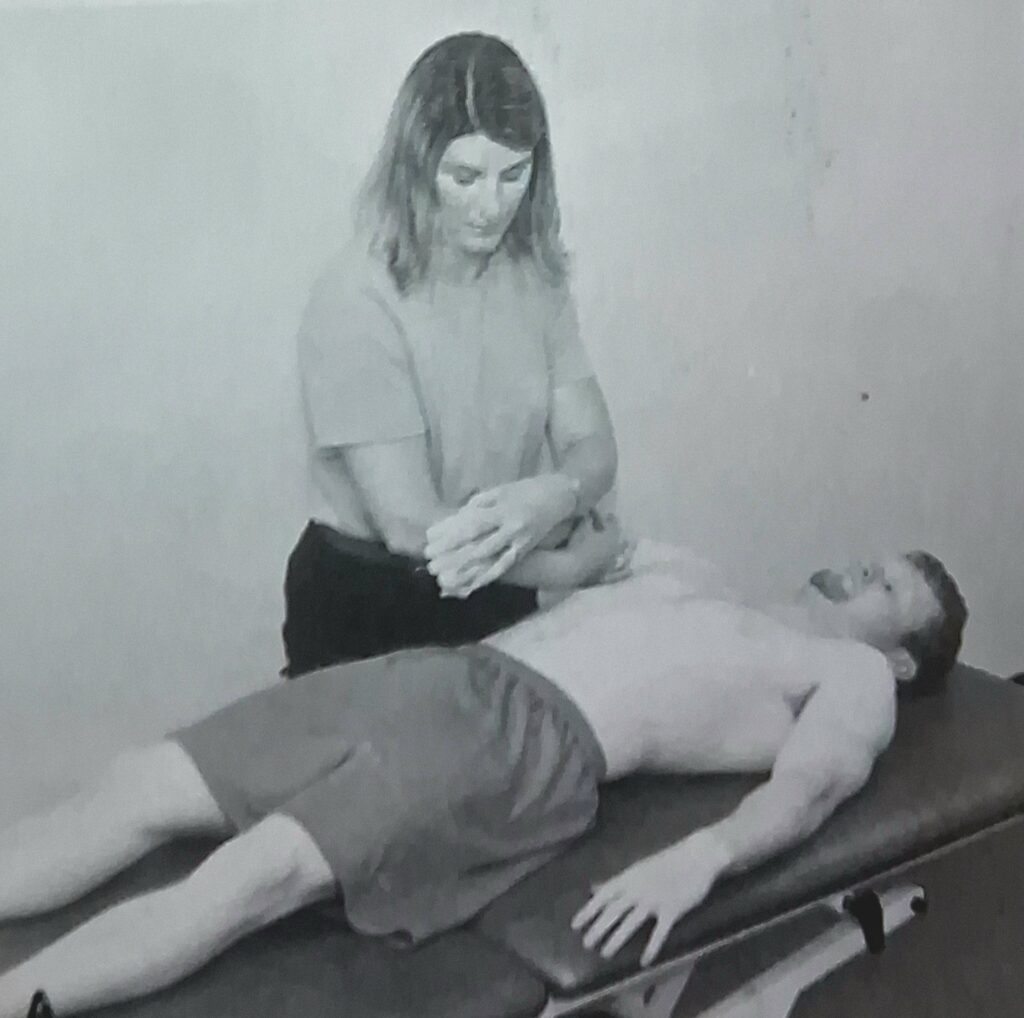
D2 Extension
Starting Position: Similar to D2 Extension in PNF pattern.
Hand placement: Place the index and middle finger of your right hand in the palm of the patient’s hand and your left hand on the volar surface of the forearm or distal humerus.
Verbal commands: ” Squeeze my fingers and pull down and across your the chest . “
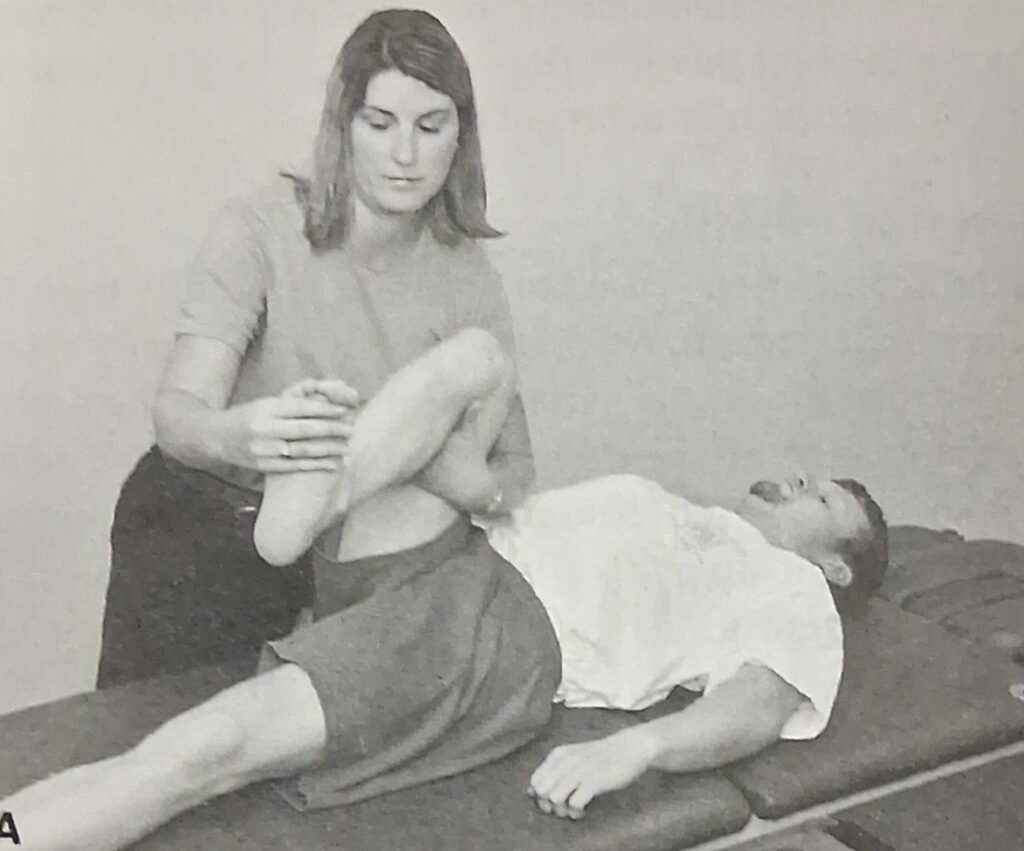
Lower Limb PNF pattern
D1 Flexion
Starting Position: Position the lower extremity in hip extension, abduction, and internal rotation; knee extension; plantar flexion and eversion of the ankle; and toe flexion.
Hand placement: Place your right hand on the dorsal and medial surface of the foot and toes and your left hand on the anteromedial aspect of the thigh just proximal to the knee.
Verbal commands: As you apply a quick stretch to the ankle dorsiflexors and inventors and toe extensors, tell the patient, ” Foot and toes up and in; bend your knee; pull your leg over and across.

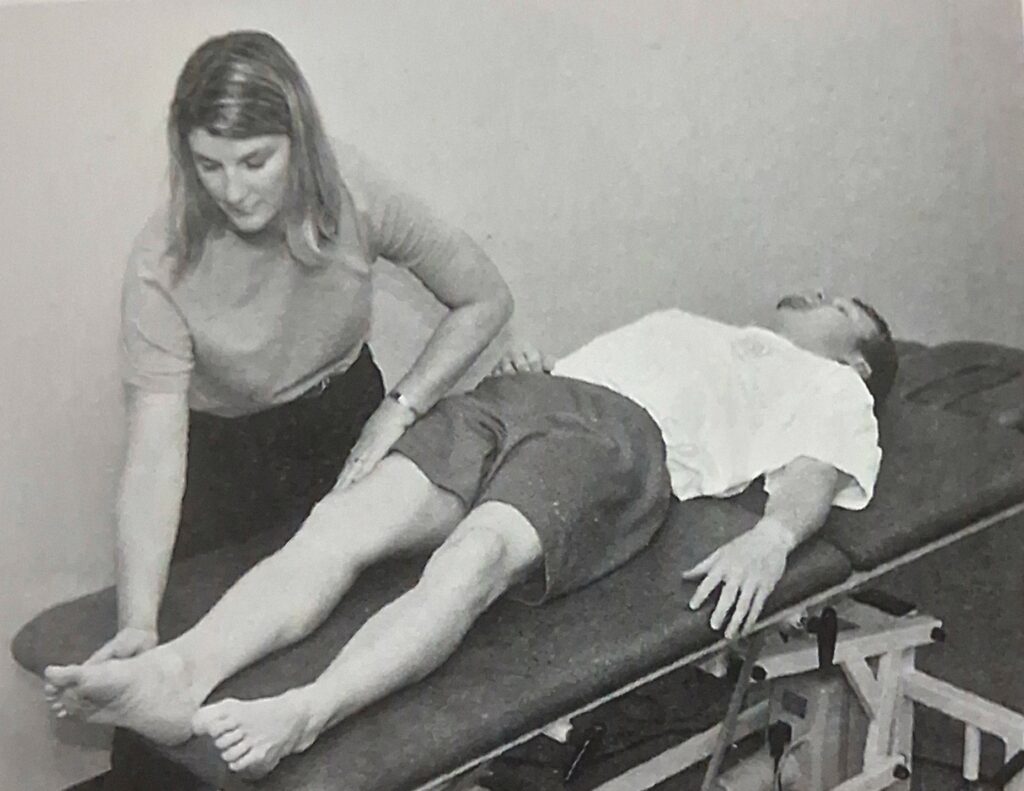
D1 Extension
Starting Position: Similar to D1 Extension in PNF pattern.
Hand placement: Place your right hand on the plantar and lateral surface of the foot at the base of the toes. Place your left hand at the posterior aspect of knee at the popliteal fossa
Verbal commands: As you apply a quick stretch to the plantar flexors of the ankle and toes, tell the patient, Curls your toes; push down and out .”
D2 Flexion
Starting Position: Position the lower extremity in hip extension, adduction, and extension rotation; knee extension; ankle plantar flexion and inversion of the ankle; and toe flexion.
Hand placement: Place your right hand along the dorsal and lateral surfaces of the foot and your left hand on the anterolateral aspect of the thigh just proximal to the knee. The fingers of your left hand should point distally.
Verbal commands: As you apply a quick stretch to the ankle dorsiflexors, evertors, and toe extensors, tell the patient, “Foot and toes up and out; Lift your leg up and out.”
D2 Extension
Starting Position: Begin as described for the completion of D2 Flexion.
Hand placement: Place your right hand on the plantar and medial surface of the foot at the base of the toes and your left hand at the posteromedial aspect of the thigh, just proximal to the knee.
Verbal commands: As you apply a quick stretch to the plantar flexors and inventors of the ankle and toe flexors, tell the patient, “Curl your toes down and in; push your leg down and in. ”