
Cranial Nerve Examination
The cranial nerve examination is the assessment of 12 cranial nerves of the body. These cranial examinations include all the motor and sensory evaluations. The cranial nerve is responsible for various functions like smell, sight, hearing, taste, and touch.

Read Related Topic Better Faster
Popular Topic Most View Most Important
Recent Release Better Bigger Faster Important
Topic
Olfactory Cranial Nerve Examination
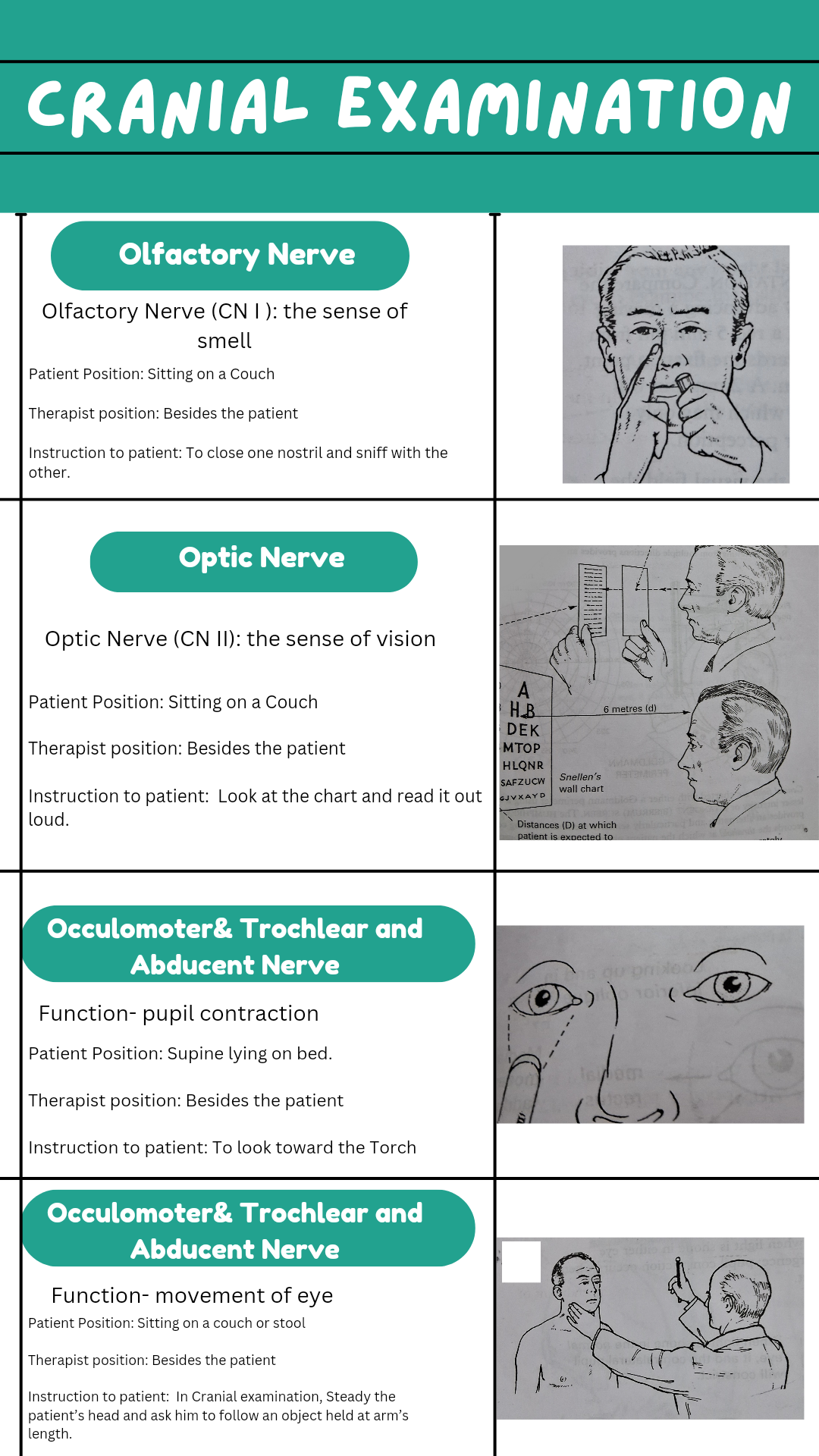
During Olfactory Cranial examination, test both perception and identification using aromatic non-irritant materials that avoid stimulation of trigeminal nerve fibers in the nasal mucosa, e.g. soap tobacco. One nostril is closed whereas the persistent sniffs with the other.
Patient Position: Sitting on a Couch
Therapist position: Besides the patient
Instruction to patient: To close one nostril and sniff with the other.
Method
Using aromatic non-irritant frequently used material can be a coffee power. The therapist will take that opened packet near one nostril separately to test the olfactory nerve.
Hypoglossal Cranial Nerve Examination
Patient Position: Sitting on a couch or stool
Therapist position: Besides the patient
Instruction to patient: Ask the patient to open their mouth; inspect the tongue
Method
Ask the patient to protrude the tongue. Note any difficulty or deviation. A protruded tongue deviates toward the side of weakness. The non-protected tongue cannot move to the opposite side. Dysarthria and dysphagia are minimal.
Optic Cranial Nerve Examination
The Optic Cranial examination is tested in each eye separately using a Jaeger-type card for near vision, labeled according to size (Normal acuity is between J1 –J4) and Snellen’s wall chart placed 6 feet away at which patient is expected to read the letter(meters).
Patient Position: Sitting on a Couch
Therapist position: Besides the patient
Instruction to patient: Look at the chart and read it out loud.
Method
Test both the near vision and far vision separately with separate charts. For near vision, doctors use Jaeger-type cards. Many doctors carry a pocket Jaeger-type card for patients in the ICU. For far vision, doctors use Snellen’s wall chart.
Note: Measure, Shape, Balance, Response to light: both understudies choke when light is shone in either eye. Response to settlement and meeting: Student narrowing happens when the look is exchanged to a near-point object.
Damage to Optic nerve
In cranial examination, a lesion of the optic nerve will abolish papillary response to light on the same side as well as in the contralateral eyes.
When light is shone in the normal eye, it and the contra lateral pupil will constrict.

Oculomotor (III),Trochlear (IV) and Abducens(VI) Nerves
Patient Position: Supine lying on bed.
Therapist position: Besides the patient
Instruction to patient: To look toward the Torch
Method
When Shine torch light is placed on the affected contralateral pupil constricts (its III nerve intact), Absent or impaired response in the illuminated eye.
When light is shone into the ordinary eye, as it were the understudy on the side constricts.
Damage to Oculomotor (III)
Ptosis: Ptosis: Ptosis is display if the eyelid hangs over the understudy when the eyes are completely open. Since the levator palpebrae muscle contains both skeletal and smooth muscle, Ptosis seen whereas performing cranial examination means either a III nerve paralysis or a thoughtful injury and is more noticeable with the former.
Ocular Movement testing
Patient Position: Sitting on a couch or stool
Therapist position: Besides the patient
Instruction to patient: In Cranial examination, Steady the patient’s head and ask him to follow an object held at arm’s length.
Method
Observe full range of horizontal and vertical eye movements.
Cranial examination of eye movement in the six different directions of gaze represents maximal individual muscle strength.
- Looking up and out superior rectus
- Looking up and in inferior oblique
- Lateral movement by lateral rectus
- Medial movement by the medial rectus
- Looking down and out inferior rectus
- Looking down and in superior oblique
Damage to Ocular Movement
Nystagmus: It is a condition in which the normal balance of eye control is upset. When the person slowly tries to drift the pupil in one direction is followed by a fast corrective movement.
Nystagmus is maximal when the eye is turned in the direction of the fast phase. Test as for other eye movements, but remember that ‘physiological ‘nystagmus can occur when the eye deviates to the endpoint of the gaze.
Trigeminal Cranial Nerve Examination
The Trigeminal cranial examination is both sensory and motor fibers tested separately.
Sensory Examination
Test For pain
Patient Position: Sitting on a couch or stool
Therapist position: Besides the patient
Instruction to patient: sit still on the stool
Method: Take a blunt pin and prick on various dermatomes of the body for the sensation of pain.
Test for Temperature
Patient Position: Sitting on a couch or stool
Therapist position: Besides the patient
Instruction to patient: sit still on the stool
Method: Take a cold object or hot /cold tubes placed on various dermatomes of the body for sensation for temperature testing.
Test for Light touch
Patient Position: Sitting on a couch or stool
Therapist position: Besides the patient
Instruction to the patient: sit still on the stool
Method: Take cotton wool and place it on various dermatomes of the body for sensation for light touch testing.
Corneal Reflex Test
Test corneal sensation by touching it with a wisp of wet cotton wools. A blink response should occur bilaterally. This cranial examination testing is the most sensitive indicator of trigeminal nerve damage
Patient Position: Sitting on a couch or stool
Therapist position: Besides the patient
Instruction to the patient: still on the stool
Method: With a wisp of wet cotton wool touch the corneal area near the eye. Normally, the person blinks bilaterally. But no blink or unilateral blink represents that there is any trigeminal nerve damage.
Motor examination
Observe for squandering and diminishing of temporalis muscle – ‘hollowing out’ the temporalis fossa.
Ask the understanding to clamp jaws together. Feel temporalis masseter muscle. Endeavor to open the patient’s jaws by applying weight to the chin. Inquire the persistent to open their mouth. If pterygoid muscles are powerless the jaw will veer off to the powerless side, being pushed over by the unopposed pterygoid muscle of the great side.
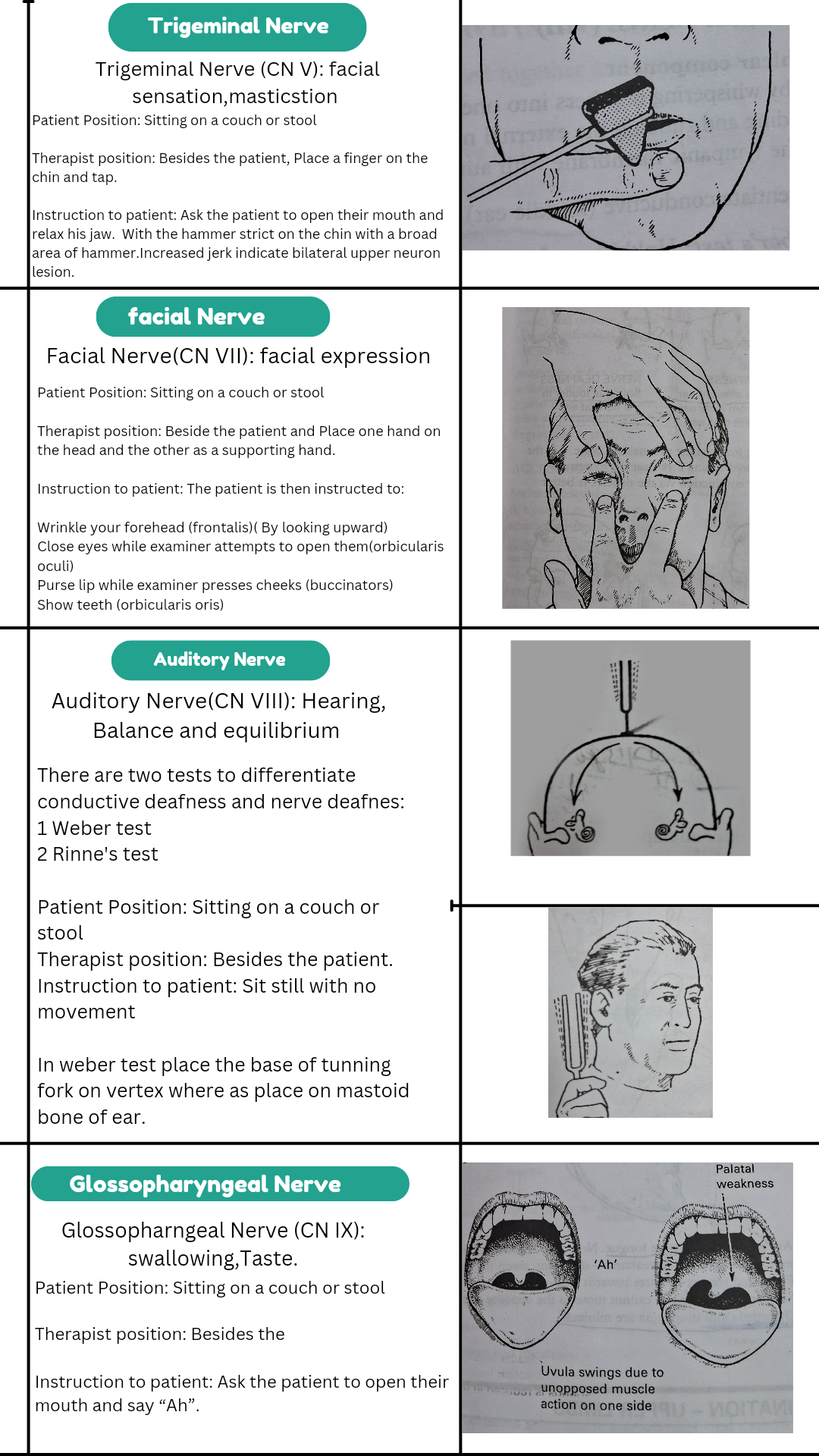
Jaw Jerk
Patient Position: Sitting on a couch or stool
Therapist position: Besides the patient, Place a finger on the chin and tap.
Instruction to the patient: Ask the patient to open their mouth and relax his jaw. With the hammer strict on the chin with a broad area of hammer :
Slight jerk: Normal
Increased jerk: bilateral upper neuron lesion.the
Facial Cranial Nerve Examination
Patient Position: Sitting on a couch or stool
Therapist position: Beside the patient and Place one hand on the head and the other as a supporting the hand.
Instruction to patient: The patient is then instructed to:
- Wrinkle your forehead (frontalis)( By looking upward)
- Close the eyes while examiner attempts to open them(orbicularis oculi)
- Purse lip while examiner presses cheeks (buccinators)
- Show teeth (orbicularis oris)
Observe the patient when he talks and smiles, watching for:
- Eye closure
- Asymmetrical elevation of one corner of the mouth
- Flattering of the nasolabial fold
Taste may be tested by using sugar, NaCl. A small quantity of each substance is placed anteriorly on the tongue.
Auditory Cranial Nerve Examination
Auditory Cranial examination has two components: cochlear is responsible for hearing and vestibular is responsible for balance and coordination.
The test is by whispering numbers separately in both ears, if hearing is impaired, examine the external meatus and the tympanic membrane with an auroscope to exclude wax or infection.
There are two tests to differentiate conductive deafness and nerve deafness
Weber test
Patient Position: Sitting on a couch or stool
Therapist position: Besides the patient.
Instruction to patient: Sit still with no movement
Hold the base of the tuning fork (512 H) strick on hand and place it against the vertex. Ask patient if the sound is heard more loudly in one ear. Normally patient will have heard the sound in both ears. In conduction deafness, sound is louder in the affected ear since distraction from external sounds is reduced in that ear. In nerve deafness, sound is the louder in the normal ear.
Rinne’s test
Patient Position: Sitting on a couch or stool
Therapist position: Beside the patient and Place one hand on the head and the other as a supporting the hand.
Instruction to patient: Sit still with no movement
Method
Take a tuning fork struck on hand and place the vibrating tuning fork against to mastoid bone. Ask the patient if the note is heard. When the note disappears -hold the tuning fork near the external meatus. The patient should hear the sound again since air conduction is better than bone conduction.
In conductive deafness, bone conduction is better than air conduction.
In nerve deafness, both bone and air conductions are impaired.
Nerve examination of the vestibular component requires specialized investigation which is called Neurotological tests.
Glossopharyngeal Nerve(IX) and Vagus Nerve (X)
These nerves are consider jointly since they are examined together and their actions are seldom individually impaired
Gag reflex testing
Patient Position: Sitting on a couch or stool
Therapist position: Besides the
Instruction to patient: Ask the patient to open their mouth and say “Ah”.
Note – Any asymmetry of palatal movement (X nerve palsy). Compare the sensitivity on each side (afferent route – IX nerve).
A positive test when there is an absent gag reflex means loss of sensation, loss of motor power, and demolish of the taste in the posterior third of the tongue (IX) is impractical to test.
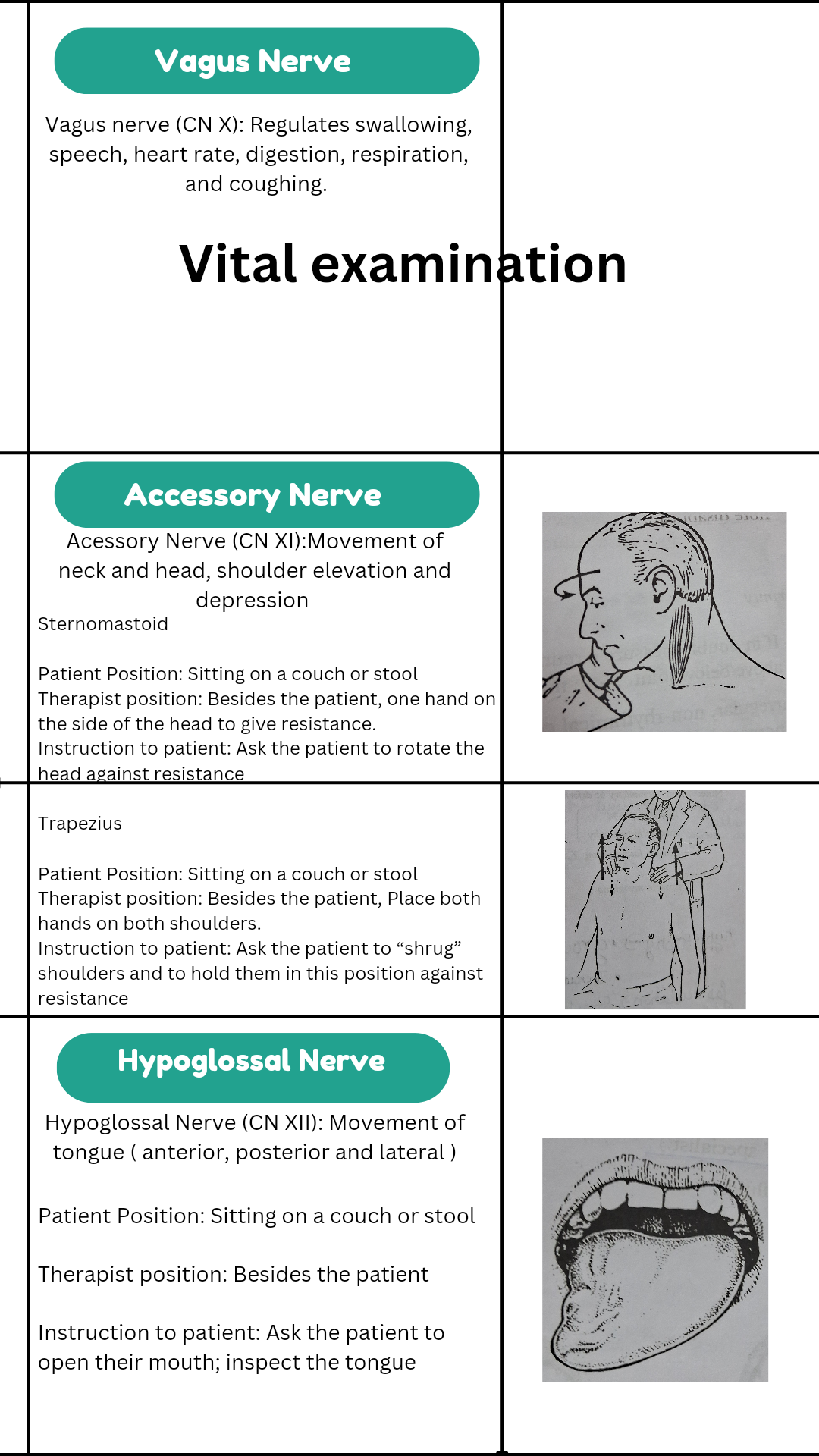
Accessory Cranial Nerve Examination
Sternomastoid
Patient Position: Sitting on a couch or stool
Therapist position: Besides the patient, one hand on the side of the head to give resistance.
Instruction to patient: Ask patient to rotate the head against resistance. Compare the power and muscle bulk on each side. Also compared each side. Also, compare each side with patient pulling the head forward against resistance. When left sternomastoid turns the head to the right and vice versa.
Trapezius
Patient Position: Sitting on a couch or stool
Therapist position: Besides the patient, Place both hands on both shoulders.
Instruction to patient: Ask the patient to “shrug” shoulders and to hold them in this position against resistance. Compare muscle power on each side. The patient should manage to resist any effort to depress shoulder.
Share With Friends
Series Topic
Muscle Manual Testing
Cranial Nerve Examination Kit



Read Related Topic Better Faster
Popular Topic Most View Most Important
Recent post Better Bigger Faster Important
Recent Posts
For sponsorship Email Us Contact Now Fill This Form
Ad@physiobia.in